The Wrist Beneath the Fingers
You sit down, extend your arm across a small cushion, and the practitioner takes your wrist between their fingers without saying a word. No form to fill out. No screen to consult. No machine humming in the background measuring something you cannot see. Just three fingers pressed lightly against the inside of your wrist, and then silence. A silence that stretches. Ten seconds. Twenty. A full minute that feels, in the particular way that being observed always does, much longer than it is. You become aware of your own breathing. You notice you have been holding something tight in your chest without realizing it. You want to explain yourself, offer symptoms, give context, perform the role of cooperative patient — but there is nothing to perform into. The practitioner’s eyes are slightly lowered, their attention turned inward toward something you cannot access from the outside. They are reading you, and you do not know what they are finding.

This is the moment that undoes most Western patients. Not pain, not fear of diagnosis, but the unbearable intimacy of being known through silence. We have spent centuries building systems of medical interpretation that require us to translate ourselves into language first — to describe, locate, quantify, narrate our suffering in ways a professional can then encode into a chart. The body, in this paradigm, is essentially a witness that must be cross-examined before it becomes legible. What the practitioner at that small cushion is doing is something categorically different. They are bypassing the testimony entirely and going straight to the evidence the body has been generating all along, without anyone asking it to.
Pulse diagnosis, in the classical Chinese medical tradition, is not a measurement of heart rate. That distinction matters enormously and is almost universally misunderstood in the West. The radial pulse at the wrist — felt across three positions on each arm, at three depths of pressure — is understood to carry information about the quality and movement of qi, the animating force that Chinese medicine has mapped across the body for more than two thousand years. The Huangdi Neijing, the foundational classical text whose compilation dates to roughly the second century BCE, devotes entire chapters to pulse as a diagnostic language, describing not merely speed but texture, width, force, rhythm, and what might be translated as the pulse’s emotional quality. Wang Shuhe, the third-century physician whose Maijing — the Pulse Classic — systematized these observations into twenty-four distinct pulse types, was not constructing metaphor. He was constructing a clinical grammar.
What modern medicine did, with extraordinary efficiency and genuine lifesaving consequence, was trade this grammar for a different one. The stethoscope, the sphygmomanometer, the electrocardiogram — each instrument extended perception while simultaneously displacing it from the body of the practitioner. The hands retreated. The machines advanced. By the time Michel Foucault analyzed the birth of the clinical gaze in his 1963 work, he was already describing something most physicians of his era would not have recognized as a loss: the reduction of the patient to a legible surface, a site of pathology to be decoded rather than a living system to be listened to. The body became an object of knowledge rather than a subject of it.
And yet the body never stopped speaking. It simply found itself in rooms where no one had been trained to hear it. The practitioner at the cushion, fingers still on your wrist, is one of the few figures in contemporary healthcare who was trained to do exactly that — to sit in the silence and let the signal arrive.
Twenty-Eight Frequencies, One Life
There is a moment in any serious encounter with classical Chinese medicine when the Western-trained mind hits a wall. Not because the ideas are obscure or mystical, but because they are too precise, too systematic, too demanding of a different kind of attention. The system of pulse diagnosis that Wang Shuhe assembled around 280 CE in his Mai Jing — the Pulse Classic — catalogues twenty-eight distinct pulse qualities, each with a name, a tactile character, a clinical meaning, and a correspondence to a particular dysfunction in the body’s internal landscape. Twenty-eight. Not a rough taxonomy, not a poetic approximation, but a rigorous classification built over centuries of accumulated observation. The floating pulse, the sunken pulse, the slippery pulse that rolls under the finger like a pearl, the choppy pulse that drags like a blade scraped across bamboo — these are phenomenological descriptions of extraordinary precision, the kind that require years of trained sensitivity to distinguish and decades to master.
The practitioner reads three positions on each wrist, known as cun, guan, and chi, each corresponding to specific organ systems. The cun position on the left wrist speaks to the heart; the guan to the liver and gallbladder; the chi to the kidney and bladder. On the right, the cun reflects the lung, the guan the spleen and stomach, the chi the pericardium and what classical texts call the triple burner — a functional relationship of energetic distribution that has no anatomical equivalent in Western medicine, which is precisely why the West found it so easy to dismiss. The pulse, in this framework, is not a measurement of cardiac output. It is a signature, a trace left by the entire dynamic system of the body’s internal weather — its excesses and deficiencies, its movements of heat and cold, its blockages and its flows.
This is where Qi must be understood with some philosophical honesty. Paul Unschuld, whose historiography of Chinese medicine remains one of the most rigorous Western engagements with the subject — Medicine in China, published in 1985, a work of genuine scholarly excavation — argues that Qi is not mysticism but a coherent epistemological framework for understanding relational energy. It is not a substance located inside things. It is the quality of interaction between things, the dynamic tension that produces observable effects. To feel a floating pulse and diagnose an exterior condition is not magic; it is pattern recognition built on a theory of how the body maintains and loses equilibrium with its environment. The Chinese medical system, Unschuld shows, was a serious intellectual tradition with its own internal logic, its own standards of evidence, its own debates and revisions across centuries. To treat it as folklore is not a scientific judgment. It is a cultural one.
The West’s dismissal of pulse diagnosis accelerated precisely during the period of colonial expansion, when European medicine became the measure of legitimate knowledge globally, not because it had proved itself superior in clinical outcomes — it had not, not yet, and in many cases not ever — but because it traveled with guns and governors. The epistemological violence of that moment is rarely discussed in medical history seminars. It is easier to say the Chinese were reading imaginary organ systems in a wrist than to acknowledge that an entire diagnostic tradition encompassing roughly two thousand years of systematic refinement was invalidated by cultural power, not clinical proof. What was dismissed was not a failure of evidence. It was a failure of translation — a failure of willingness, which is something else entirely.
The pulse, meanwhile, kept beating. Twenty-eight ways of being alive, twenty-eight frequencies of internal weather, waiting for a hand trained enough to listen.
What Silence Diagnoses
There is a man who wakes every night at exactly three in the morning. Not with a gasp, not from a nightmare with a recoverable narrative — simply awake, in the dark, his chest already tight with something that has no name and no address in the body. He lies still. His heart rate is normal. His blood pressure, when he finally checks it, is unremarkable. By morning he functions well enough that no one around him suspects a thing, and by the time he sits across from a physician he cannot describe what happened because clinically, provably, nothing happened. The instruments agree.
This is precisely the territory that Arthur Kleinman mapped with such uncomfortable precision in his 1988 work “The Illness Narratives,” where he drew the distinction — radical at the time, still largely ignored in practice — between disease as the measurable biological deviation and illness as the lived experience of suffering. Western clinical medicine, he argued, was structured to treat the former while systematically dismissing the latter. The patient leaves with bloodwork that shows nothing and a vague sense of having been told they are inventing themselves.
Then there is a woman whose hands tremble — but only in one specific moment. Not during the commute, not during the long meetings, not even during the arguments she has rehearsed into smoothness. Her hands tremble only when she is on the verge of saying something true. Something that costs her. The tremor arrives like a warning from a part of herself she has been outrunning for years. No neurologist would catch it because no neurologist would be in the room for the right silence.
The anthropologist Thomas Csordas, writing in the early 1990s on what he called the paradigm of embodiment, argued that the body is not a container for experience but the very site of culture — that what we carry socially, we carry somatically. The body does not metaphorize. It literalizes. Kleinman’s somatization, in this light, is not a failure of the psyche to communicate properly; it is the psyche communicating with devastating accuracy through the only language that cannot be politely edited.
Pulse diagnosis in classical Chinese medicine enters here not as mysticism but as method — a method designed precisely for this bandwidth of information that Western diagnostics structurally cannot receive. The Liver pulse that rises too forcefully under the fingers, or the Kidney pulse that feels deep and almost absent, is not describing a pathology in any biochemical sense. It is describing a pattern of relationship — between the person’s inner state and the performance they are sustaining for the world. Between what is felt and what is shown. The dissonance between these two things, held long enough, becomes the precondition for illness before illness has a name that any machine can confirm.
Kleinman himself noted that the biomedical model treats the body as a malfunctioning mechanism and the doctor as a repair technician — a metaphor so embedded in medical education that it shapes what physicians are even capable of noticing. What gets filtered out is precisely what pulse diagnosis was refined over centuries to detect: not the organ, but the orientation of the person inside the organ. Not the symptom, but the direction of force that is producing it.
The man who wakes at three in the morning is not suffering from insomnia in any clinically actionable sense. He is suffering from a life organized around suppression. The woman whose hands betray her has a body that is more honest than she has been permitted to be. Both of them would arrive at a Western clinic and leave with a clean bill of health. Both of them, under a trained hand reading the pulse, would tell an entirely different story without saying a single word.
The Body That Preceded the Self
There is a moment, familiar to almost everyone, when you realize your jaw has been clenched for hours. Not tense — clenched. Molars pressed against molars with a force that borders on fury, and you had no idea. The tension was there before the awareness of it, living in the tissue, running its own quiet program while you answered emails and made dinner and told someone you were fine. The body was speaking. You were not listening. You were, in fact, not even in the room.
This is not a failure of attention. It is the structural consequence of an inheritance most of us never chose — a way of inhabiting ourselves that was built over centuries and handed to us as though it were simply the truth of what a person is.
Maurice Merleau-Ponty spent the better part of his philosophical life trying to dismantle the idea that the body is something we have, as opposed to something we are. In his Phenomenology of Perception, published in 1945, he argued that the body is not an object among objects, not a vehicle the mind pilots toward its destinations. It is the primary site of being-in-the-world — the condition of all experience, prior to reflection, prior to language, prior to the construction of any self that could stand apart and observe. Perception does not happen in the mind and then get reported by the body. Perception is bodily, all the way down, before any thought has had the chance to form.
The pulse, understood through this lens, is not a symptom the body produces for the mind to interpret. It is something closer to the body’s own awareness of itself — a pre-subjective signal, a rhythm that precedes identity the way breathing precedes the decision to breathe. When a classical practitioner places three fingers along the radial artery and reads what they find there, they are not collecting data about an object. They are entering into a conversation with a subject that has been speaking long before the person lying on the table had words for any of it.
The violence of losing access to that conversation is real, and it has a history. René Descartes drew the line clearly in the seventeenth century — mind on one side, extended matter on the other — but it was the institutionalization of clinical medicine in the nineteenth century that made the split structural and enforced. When hospitals reorganized knowledge around pathological anatomy, around the lesion visible to the dissecting eye, the body became a territory to be mapped from outside. The patient’s felt experience became, at best, a clue pointing toward the real evidence. At worst, it became noise. What could not be measured could not be trusted, and what could not be trusted could not be treated.
Pulse diagnosis did not simply become unfashionable within this paradigm. It became literally unthinkable — a category error, the confusion of subjective impression with objective fact. To suggest that the quality of a rhythm under the fingertips could carry information about grief, or exhaustion at a level below fatigue, or the early stirring of a disease not yet visible on any scan, was to speak a language the institution had decided was not a language at all.
And so an entire mode of bodily self-knowledge was not refuted so much as rendered invisible. The person who arrives at a clinic describing a feeling they cannot name, a wrongness that has no location, learns quickly to translate that experience into a form the system can process, or to stop describing it altogether. The body keeps speaking. The institution was not designed to hear it.
What gets lost in that silence is not just diagnostic information. It is the recognition that something in you knew before you did.
The Practitioner’s Attention as Medicine
You are back in that room. The same low light, the same stillness that feels almost transgressive in a world that has monetized every minute of human contact. The practitioner’s fingers return to your wrist, and this time you understand that what is happening is not primarily diagnostic. The three fingers pressing gently into the radial pulse are not searching for data points. They are doing something rarer and more destabilizing than that: they are paying attention to you — to all of you, the whole complicated system of you — without any intention of moving on quickly.
This is what modern healthcare has quietly, systematically, and perhaps irreversibly eliminated. The average general practitioner appointment in the United Kingdom runs to 9.2 minutes as of 2023, a number that has not meaningfully grown despite decades of evidence showing its inadequacy. In the United States, a physician is physically present in the consultation room for less than half of an eighteen-minute appointment, the remainder consumed by screens and documentation, by the architecture of throughput disguised as care. These are not statistics about inconvenience. They are statistics about what we have collectively decided a human being is worth, expressed in the currency of attention.
Simone Weil, writing in what would become “Waiting for God,” published posthumously in 1951, argued that attention in its purest form is the rarest and most generous act one person can offer another. Not effort, not expertise, not solution — attention. She described it as a kind of emptying, a willingness to receive the reality of another person without immediately filling that space with one’s own agenda, one’s own categories, one’s own need to conclude. For Weil, this quality of attention was not passive. It was the most demanding thing a human being could do, precisely because it required the suspension of the self’s constant forward motion. The practitioner with three fingers on your wrist is doing exactly this. They are not moving forward. They have stopped, genuinely stopped, in a way that the nine-minute appointment structurally forbids.
What pulse diagnosis restores, then, is not an ancient technology competing with modern diagnostics. It restores the therapeutic act of being fully witnessed. There is a growing body of research, largely emerging from psychoneuroimmunology since the 1980s, suggesting that the experience of feeling genuinely seen by another person produces measurable physiological shifts — in cortisol levels, in heart rate variability, in immune markers. The healing is not only in the diagnosis. Some portion of it lives in the quality of the encounter itself, in the willingness of one consciousness to make space for another without the tyranny of the clock dismantling that space before it can form.
The practitioner reads your pulse in three positions on each wrist, at three depths of pressure, over a span of time that would seem wasteful in a hospital corridor. They are not wasting time. They are refusing to treat time as the primary value in the transaction, and that refusal is itself a form of medicine that cannot be replicated by any instrument yet built, however precise.
Which brings you to the question you cannot quite close the door on: if we have always known, in the oldest and most visceral part of ourselves, that to be truly attended to is to begin to be healed — if every tradition of care across every culture has encoded this knowledge in its rituals and its gestures and its deliberate slowing down — then the real question is not why pulse diagnosis survives, but whose interests were served by convincing us to forget it, and whether the agreement to forget was ever something we consciously chose, or simply something that was chosen for us while we were not paying attention.
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision
🌿 Ancient Energy: Channels, Rhythms & the Living Body
Pulse diagnosis is just one doorway into the vast landscape of traditional energetic medicine. These related articles deepen your understanding of how ancient traditions mapped the invisible forces that animate us, from the meridian system to the cyclical rhythms of organ energy throughout the day.
The 12 Energetic Channels: The Secret Map of Meridians in Body
If pulse diagnosis listens to the river, the meridians are its banks. This article traces the twelve energetic channels that form the hidden architecture of the body, revealing how Qi flows along precise pathways that connect organs, emotions, and the outer world. Understanding this map transforms pulse reading from a diagnostic tool into a living conversation with the body’s deepest intelligence.
GO TO THE SELECTION: The 12 Energetic Channels: The Secret Map of Meridians in Body
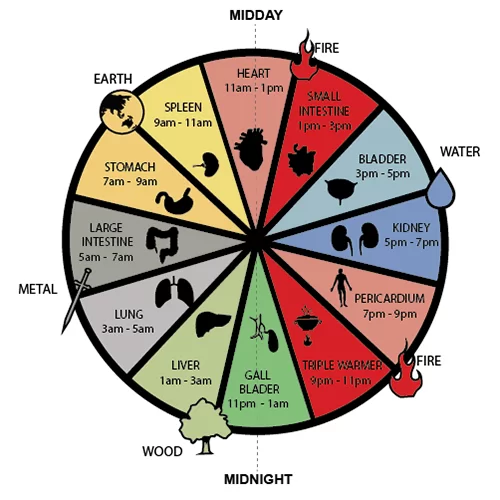
The Organ Clock: Why Every Organ Has Its Time of Peak and Low Energy
Pulse diagnosis captures a snapshot of Qi in motion, but the Organ Clock reveals that this motion follows a strict daily rhythm. Each organ surges with peak energy during a two-hour window and recedes into its trough twelve hours later, creating a biological symphony that ancient physicians learned to read alongside the pulse. Knowing this clock allows practitioners to interpret not just how Qi is distributed, but when the body is most vulnerable or most alive.
GO TO THE SELECTION: The Organ Clock: Why Every Organ Has Its Time of Peak and Low Energy
Vital Breath: if Your Qi is Blocked, Weak, or Scattered
What the pulse ultimately measures is the quality and coherence of Qi itself — whether it flows freely, stagnates, or disperses without direction. This article explores the three fundamental dysfunctions of Vital Breath: blockage, weakness, and scattering, each of which leaves a distinct imprint on the pulse under a skilled practitioner’s fingertips. Together, these concepts form the diagnostic grammar that makes ancient pulse reading a precise and nuanced clinical art.
GO TO THE SELECTION: Vital Breath: if Your Qi is Blocked, Weak, or Scattered
Zheng Qi: How to Nourish Upright Energy to Protect Against External Pathogens
Zheng Qi, or Upright Energy, is the body’s sovereign force of self-protection and integrity, and pulse diagnosis is one of the primary tools for assessing its strength. When Zheng Qi is abundant and well-nourished, the pulse carries a quality of resilience that traditional physicians associated with immunity and vitality. This article explores the practices and principles behind cultivating this foundational energy, offering a natural companion to the deeper understanding of what your pulse is truly communicating.
GO TO THE SELECTION: Zheng Qi: How to Nourish Upright Energy to Protect Against External Pathogens
Discover the Cinema of the Soul on Indiecinema
The same curiosity that draws you toward ancient wisdom and invisible energies has always found its mirror in independent cinema. On Indiecinema streaming you will find films that dare to explore consciousness, healing, and the mysteries of existence with the same depth and sincerity. Come discover a curated world of visionary independent movies that speak directly to the seeking mind.
👉 EXPLORE THE CATALOG: Watch Indie Films in Streaming
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision

