The body as a site of social inscription
You are sitting in a chair that was clearly chosen for its neutrality — beige, wipeable, neither comfortable nor deliberately uncomfortable — and the doctor is saying a number, a count, a ratio, something measurable about your blood, and you realize in that exact moment that your body has just changed jurisdiction. Not biologically. Administratively. The cells were already doing what they were doing before anyone named them. But the naming is what relocates you. From this point forward, your body is no longer primarily yours. It is a case, a file, a reportable condition under public health statutes that vary by country but share a common grammar: the grammar of containment.

What happens in that room is not merely medical. It is a form of social inscription so total that most people who live through it describe it not as receiving information but as becoming something different. The distinction matters. Information can be processed, contextualized, filed away. Becoming is irreversible in a specific register — it changes not what you know but what you are assumed to be by every institution you will subsequently encounter. Insurance actuaries, immigration officers, sexual partners, family members who find out by accident or by necessity all receive a version of you that was written in that beige room, by a number spoken aloud, before you had any language to resist it.
Michel Foucault spent considerable energy in The Birth of the Clinic, published in 1963, tracing the moment when the modern body became a legible object for medical power — a surface to be read rather than a person to be heard. What he identified was not conspiracy but structure: the clinic reorganized perception itself, training the gaze to see through the person toward the pathology beneath. The body became, in his framing, both subject and object of knowledge simultaneously, which sounds philosophical until you are the one sitting in the beige chair and realizing that every question being asked of you is in fact a question being asked about your body as evidence.
HIV accelerated this dynamic into something the medical humanities had not fully theorized before the epidemic forced the issue. When the first case definitions were published by the CDC in 1981, the disease was named by who was dying, not by what was causing the deaths. The original surveillance language clustered cases under the acronym GRID — Gay-Related Immune Deficiency — before the science caught up with the social panic already structuring the response. The body infected with HIV was, from the very beginning of the epidemic’s public life, a body already pre-inscribed with social meaning. To receive the diagnosis was to inherit that history whether you wanted it or not, whether you shared any of its demographic markers or not.
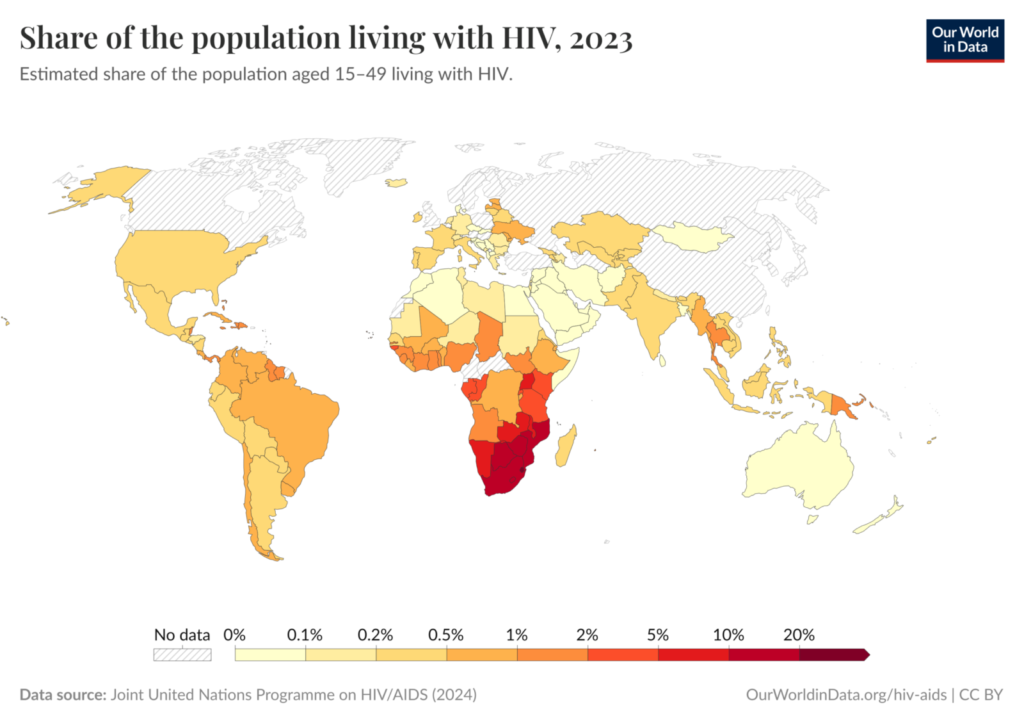
Susan Sontag, in Illness as Metaphor published in 1978 and its sequel AIDS and Its Metaphors a decade later, argued with surgical precision that certain diseases attract moral narratives the way wounds attract infection — not because of anything inherent to the biology, but because of the cultural anxiety that finds in illness a convenient allegory. AIDS became an allegory for transgression, for excess, for what happened to people who had stepped outside the boundaries of normative behavior. The allegory was so powerful that it survived every piece of evidence that contradicted it, including the millions of heterosexual transmissions in sub-Saharan Africa, the infected children, the contaminated blood supplies in France whose scandal in 1985 implicated the national health ministry directly. The metaphor was not updated by the facts. The facts were absorbed into the metaphor.
This is what the body becomes after diagnosis: a location where several incompatible stories are being told at once, and none of them were written by the person inside it. The medical story, the legal story, the moral story, and the identity story all converge on the same flesh, and the person living in that flesh is handed the task of negotiating between narratives that were never designed to accommodate their actual experience.
The 1980s script that never ended
You already know the image before I describe it. The gaunt face. The hospital bed. The lesions. The candlelight vigil. The quilt panel with a name stitched in fabric by someone who could barely see through their grief. These images arrived in the 1980s with the force of emergency broadcast signals, and the cultural nervous system has never fully switched them off, because emergencies of that magnitude do not end — they sediment.
Between 1981 and 1995, the United States alone recorded more than 300,000 AIDS-related deaths. In those years, the Reagan administration’s studied silence — Reagan did not publicly address AIDS until 1987, six years into the epidemic — created a vacuum that culture rushed to fill. What filled it was catastrophe iconography: Susan Sontag, writing in 1989 in “Illness as Metaphor and AIDS and Its Metaphors,” identified how AIDS attracted the metaphorical vocabulary of invasion, pollution, and punishment with a speed and ferocity that exceeded even the language previously grafted onto cancer. The disease became a moral statement before it was fully understood as a biological one. And moral statements, unlike viral mechanisms, do not respond to treatment.
The pharmaceutical rupture came in 1996, when combination antiretroviral therapy — the protease inhibitor cocktail — produced what researchers called the Lazarus effect: patients who had been preparing to die stabilized, recovered, returned to their lives. Within two years, AIDS-related mortality in wealthy countries dropped by more than sixty percent. This was not a minor adjustment to an existing narrative. It was a biological discontinuity so complete that the story humanity had been telling about HIV simply became factually false. People with HIV who have access to treatment and maintain an undetectable viral load do not transmit the virus sexually — a finding confirmed definitively by the PARTNER2 study in 2019, which tracked 972 male couples over eight years and recorded zero linked transmissions. Zero. The science had left the cultural imagination standing at the graveside of a funeral that no longer needed to happen.
But culture does not update itself on the schedule of clinical trials. The 1980s template had been too catastrophic, too visceral, too thoroughly woven into the grammar of how Western societies processed sex, death, and transgression. Erving Goffman’s work on stigma — specifically his 1963 analysis of how society reduces individuals to a single spoiled identity — anticipated precisely this dynamic: once a condition becomes the primary lens through which a person is perceived, no subsequent information about that person easily penetrates the lens. The diagnosis becomes the biography. The historical moment of maximum death becomes the permanent present tense.
What this produces in lived experience is a particular form of temporal dislocation. Someone diagnosed with HIV in 2024, placed on treatment and rendered undetectable within weeks, must nonetheless negotiate with a cultural ghost — the emaciated body, the stigmatized community, the death sentence — that has no relationship to their actual medical situation but enormous power over every social interaction that follows. Their doctor may speak the language of 2024. Their employer, their family, their potential partner may still be fluent only in 1987. This gap is not metaphorical suffering. It is the mechanism by which a treatable chronic condition continues to function as a social catastrophe decades after it ceased to be an inevitable biological one.
The activist group ACT UP understood, during the worst years, that visibility was itself a political act — that dying in public was the only way to force an indifferent government to look. They were right, and they saved lives. But the images they burned into collective memory also burned a permanent association between HIV and dying that no subsequent press release about undetectable viral loads has managed to fully extinguish.
Undetectable as an epistemological rupture
You sit across from someone you trust, maybe even love, and you say the words carefully, watching their face for the shift you already know is coming. The science is clear, you have explained it twice now, the viral load is undetectable, transmission is not possible, the studies followed nearly two thousand serodiscordant couples across fourteen European cities for years, recording zero linked transmissions. None of this lands. The face does not change because of the data. It changes, or rather it refuses to change, because the information is arriving inside a room that was built before the information existed.
This is what an epistemological rupture actually feels like from the inside — not the clean revolution of a Kuhnian paradigm shift happening at the level of institutions and textbooks, but the specific friction of a fact that is scientifically settled and socially inadmissible at the same time. The PARTNER studies, published in their full scope in 2019 in the Journal of the American Medical Association, produced something unusual in public health: a mathematical certainty. Zero transmissions. Not a reduced risk. Not a negligible probability. A null result in conditions of real sexual life, not laboratory modeling. The researchers were explicit. The evidence was, by the standards of any comparable epidemiological work, conclusive. And yet the social architecture surrounding HIV did not receive this finding the way it would have received, say, updated guidelines on cholesterol thresholds.
Stigma has always been studied as if it were a lag, a delay between what science knows and what culture believes, as though given enough time and enough education campaigns, the distance would close. This is almost certainly wrong. Susan Sontag, writing in 1988 in Illness as Metaphor, identified something more structurally disturbing: that certain diseases are recruited into moral narratives that precede them and will outlast any particular medical fact about them. The illness becomes a language for speaking about punishment, transgression, invisible threat, deserved suffering. Once that grammar is installed, correction at the level of virology is insufficient because the thing being corrected is not a belief about transmission rates. It is a belief about who certain people are.
The U=U paradigm threatened to collapse an entire symbolic architecture that had been under construction since the early 1980s. What it offered was not merely reassurance to people living with HIV. It was an ontological reclassification — a person with an undetectable viral load is not, in any medically meaningful sense, a vector of disease. The category that had organized four decades of fear, policy, legal prosecution, and intimate rejection simply ceased to apply. Several American states still maintain criminal statutes that can convict a person for potential exposure even when transmission was scientifically impossible. As of 2023, fewer than half of U.S. states had modernized their HIV criminalization laws to account for current science. The law, in those jurisdictions, is not behind the science. It is actively defending a prior version of reality against the current one.
What this reveals is that scientific consensus, even when it is unambiguous, does not automatically inherit the social authority of the beliefs it displaces. Knowledge and legitimacy are not the same currency. A fact can be true and still be refused admission into the rooms where it most needs to operate — the bedroom, the courtroom, the family dinner table, the psychiatric intake form that asks about risk behaviors without asking about viral load. The gap between what is demonstrably real and what is socially permitted to count as real is not ignorance. It is a choice, distributed across thousands of small daily decisions by people who prefer the older story because the older story does something for them that the new one refuses to do.
It organizes their fear into someone else’s body.
Disclosure as a political act imposed as a personal duty
You rehearse the conversation in your head for weeks before it happens. You choose the words carefully, then discard them, then choose them again. You consider the lighting, the timing, the exact emotional temperature of the person across from you. And somewhere beneath all of that preparation, beneath what looks like intimacy and courage, sits a threat you did not invent and cannot escape — the threat that if you do not speak, the law may speak for you.
More than sixty countries currently maintain criminal statutes that can prosecute a person living with HIV for failing to disclose their status to a sexual partner, even in cases where transmission is biologically impossible — where viral suppression renders the individual non-infectious, where condoms were used, where no transmission occurred and none could have. The science absorbed by medicine twenty years ago has not been absorbed by law. The landmark PARTNER and PARTNER2 studies, completed between 2010 and 2018 across fourteen European countries and involving nearly 1,200 serodifferent couples, produced zero transmissions from partners with an undetectable viral load. Zero. Law, in most jurisdictions, continues to operate as though these numbers do not exist.
What this architecture produces is not protection. It produces a compulsory theater of confession in which the person living with HIV bears alone the moral and legal weight of a public health failure that belongs to everyone. The state invested inadequately in sexual education for decades, allowed stigma to calcify into policy, permitted testing infrastructure to remain fragile and inaccessible — and then redirected the responsibility for managing all of that failure onto the individual body that carries the virus. Criminal disclosure law is not a public health instrument. It is a displacement mechanism, transferring structural debt onto personal biography.
The sociologist Goffman, writing in 1963 in Stigma: Notes on the Management of Spoiled Identity, described how societies construct categories of the discreditable — those who carry attributes that, once known, fundamentally alter how others perceive and treat them. The disclosure demand does not merely ask for honesty; it demands that a person announce their membership in a stigmatized category before any intimacy can proceed legitimately. The law, by inserting itself into that moment, transforms a private negotiation into a juridically loaded act, one where the wrong answer carries potential imprisonment. In Canada, individuals have been prosecuted and convicted under aggravated sexual assault statutes for non-disclosure even when their viral loads were undetectable — a legal reality that organizations like the Canadian HIV/AIDS Legal Network have spent years attempting to dismantle, with only incremental success.
What disappears inside this framework is any serious conversation about shared responsibility. Partners who decline to test, who prefer not to know, who actively resist conversations about sexual health — they carry no equivalent legal obligation. The asymmetry is not incidental. It maps precisely onto older logics of contagion and blame, the same logics that in 1987 allowed William Dannemeyer to argue before the United States Congress that HIV carriers should be registered as public health threats, language that preserved the grammar of pollution for people rather than viruses. The criminal law that followed in various forms across the following two decades did not emerge from epidemiological evidence. It emerged from that grammar.
There is also a quieter violence in the demand, one that operates below the threshold of prosecution. The person who discloses and is met with rejection, disgust, or exposure to others learns something about the cost of honesty that no statute was designed to offset. The person who does not disclose lives inside a different kind of siege, waiting for the moment when the secret becomes evidence. Both of these are states of sustained psychological injury, and neither of them is a product of the virus itself — they are products of a social order that chose punishment over literacy, disclosure mandates over genuine collective education about what transmission actually requires.
The pharmaceutical narrative of rescue and its costs
You take the pill at the same time every day, sometimes with breakfast, sometimes slipped into a pocket for later, and after a while the gesture becomes so ordinary that you forget, briefly, that the thing you are managing has a name at all. That forgetting is partly the point. The pharmaceutical industry, the public health apparatus, and the popular press collaborated across the 2000s and 2010s to produce one of modern medicine’s most genuinely extraordinary stories: a virus that had killed hundreds of thousands annually was brought, through antiretroviral therapy, to something resembling biological silence. By 2021, the World Health Organization reported that approximately 28.2 million people were accessing treatment globally. One pill. Once a day. A near-normal life expectancy. The headline wrote itself, and once written, it functioned as a kind of permission to stop asking further questions.
The philosopher of science Ian Hacking, in his 1999 work “The Social Construction of What?”, described how categories of illness are never neutral containers — they reshape the people held inside them, and the stories told about those categories reshape what those people are allowed to feel. When the dominant narrative around HIV became a story of pharmaceutical rescue, the experience of living inside that rescue quietly lost its legitimacy as a subject worth investigating. The medical problem had been solved. What remained — the dread that precedes each annual blood draw, the arithmetic of disclosure that governs every new relationship, the fatigue that is not quite fatigue and has no diagnostic code — became, by implication, a personal failure to update one’s emotional software accordingly.
What the biomedical success genuinely achieved was profound and should not be minimized: it removed death as an imminent horizon for millions of people. But the removal of death is not the same as the installation of life, and confusing the two has had measurable costs. Research published in journals including “AIDS and Behavior” through the 2010s documented rates of depression among people living with HIV running two to three times higher than in the general population — figures that did not improve proportionally as treatment became more effective. The pill suppressed the virus; it did not suppress the stigma internalized years before the prescription was written, the shame that had already restructured a person’s relationship to their own body, their expectations of intimacy, their sense of whether they were someone to whom good things were permitted to happen.
The economic architecture of treatment further complicates the rescue narrative in ways that rarely surface in the triumphalist accounts. Gilead Sciences reported revenues exceeding 24 billion dollars in 2022, with HIV medications constituting a substantial portion of that figure. The one-pill-once-a-day formulation is both a clinical marvel and a commercially optimized delivery mechanism that requires indefinite consumption. The patient who achieves an undetectable viral load is not cured — they are retained, durably, within a pharmaceutical relationship that demands daily compliance, insurance continuity, and in many healthcare systems, significant out-of-pocket exposure. For people living in countries where treatment access depends on donor funding cycles, geopolitical relationships, or the administrative caprice of public health bureaucracies, the promise of near-normal life expectancy exists less as a lived reality than as a statistical average aggregated across conditions most individuals never fully inhabit.
Sociologist Steven Epstein, writing in “Impure Science” in 1996, traced how AIDS activism fundamentally altered the epistemology of clinical research — patients became credible knowledge producers, their experiential testimony forcing its way into methodological frameworks that had previously excluded it. What happened in the decades after that victory is that the experiential testimony was welcomed precisely as long as it confirmed the efficacy of treatment, and sidelined the moment it began to describe something treatment could not reach.
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision
Intimacy under surveillance

She has rehearsed this sentence four hundred times. In the shower, in the car, in the half-second before sleep arrives. The words have been arranged and rearranged so many times they no longer sound like language — they sound like a liability waiver, a medical disclaimer, something you sign before boarding for a high-risk activity. And yet when the moment arrives, when the person across the table leans forward and the air between them changes quality, her throat closes around the rehearsed sentence like a fist around water.
What she is experiencing is not simply nervousness. It is the internalized structure of a verdict that was handed to her by every silence, every recoil, every news cycle that used her diagnosis as metaphor for moral failure. Erving Goffman, in Stigma: Notes on the Management of Spoiled Identity, published in 1963, identified this precisely — the moment when a person with a concealable stigma must calculate, in real time, whether to disclose or pass, and how that calculation colonizes every interaction until authenticity becomes structurally impossible. The self splits: there is the self who sits at the table and the self who watches from above, running probability models on rejection. This bifurcation is not a psychological malfunction. It is a rational adaptation to an irrational social environment.
The particular cruelty of HIV stigma in intimate contexts is that it arrives pre-loaded with a history the other person carries without knowing they carry it. Decades of public health messaging built around fear — the campaigns of the 1980s that used skulls and tombstones and the language of plague — did not disappear when antiretroviral therapy transformed HIV into a manageable chronic condition. They sediment. They become the inherited furniture of the cultural unconscious, and no amount of updated statistics dismantles furniture that was installed before most people now dating were born. The Undetectable Equals Untransmittable consensus, confirmed by the PARTNER studies concluding in 2019 after tracking nearly 1,000 serodiscordant couples through 77,000 condom-free sexual encounters with zero linked transmissions, does not reach the person at that table with the same velocity as thirty years of catastrophic imagery.
So what she discloses is never just a medical fact. She discloses into a pre-existing narrative she did not author and cannot fully control. The sentence she has rehearsed must somehow carry the weight of correcting that narrative, managing the other person’s fear, protecting her own dignity, and leaving space for the connection she actually came here for — all simultaneously, in the span of a breath. Researchers studying disclosure among people living with HIV have documented what they call “identity threat anticipation,” a cognitive posture so chronic it begins to reshape how people narrate themselves to themselves, not just to others. The anticipated rejection loops backward into self-conception until some people describe feeling the need to apologize for existing in desirable forms, as though desire itself had become a trespass.
There is something worth sitting with in the way intimacy has become, for millions of people, a site of labor that is entirely invisible to their partners. The emotional work performed before a conversation begins, the calibration of timing and setting and phrasing, the strategic deployment of medical vocabulary to preempt panic — none of this registers as work in any cultural ledger. It is simply expected, quietly demanded, absorbed into the body of the person who lives with the diagnosis as though it were a natural cost of entry into human connection rather than a tax levied by a social world that still cannot look at the virus without reaching for its oldest stories about bodies that contaminate, people who transgress, desire that punishes.
What does it do to a person to spend years perfecting a sentence whose only purpose is to ask permission to be wanted?
Identity capture and the tyranny of the chronic condition
You are handed a diagnosis and, without ceremony, a new identity. Not a supplement to the one you carried in — not an addendum — but a replacement architecture, quietly installed while you were still processing the word your doctor had just said aloud.
Arthur Kleinman spent decades drawing a line that medicine kept refusing to honor: the line between disease, which belongs to the biological organism and its measurable dysfunctions, and illness, which belongs to the person living inside that organism — the suffering shaped by meaning, by relationships, by the stories a culture tells about what is happening to a body and why. His 1988 work The Illness Narratives argued that clinical medicine, in its relentless focus on pathology, consistently amputates the second category in order to manage the first. The result is not neutral. When the illness — the lived, interpreted, socially embedded experience — is stripped away in favor of pure disease management, the person does not disappear. They are simply left to construct their identity in a vacuum, with no framework except the medical one handed to them at diagnosis. And that framework is totalizing. It does not leave room for nuance. It says: this is now the organizing fact of your existence.
Erving Goffman noticed something about the mechanics of social identity that feels almost too precise to be theoretical. In Stigma, published in 1963, he described how certain attributes — visible or eventually disclosed — do not merely add to a person’s social profile but effectively overwrite it. He called this a “spoiled identity,” and what he meant was not that the person becomes worthless but that they become unreadable except through the attribute that marks them. Every other quality they possess — their intelligence, their tenderness, their professional competence, their humor — gets reprocessed through the stigmatized fact, either dismissed or reinterpreted as a function of it. The person ceases to be a subject with a condition and becomes, in the social imagination, a condition that incidentally contains a person.
HIV has never been a neutral diagnosis in this sense. Its arrival in the early 1980s was accompanied by a specific cultural grammar that fused the medical fact with moral meaning, with behavioral accusation, with a verdict on who deserved what. That grammar did not vanish with the development of antiretroviral therapy. It migrated. It became subtler, embedded in the pauses before disclosure, in the careful calibration of who gets told and who does not, in the hypervigilance that shapes every new intimacy. A person managing a well-controlled viral load — undetectable, non-transmissible — still carries the weight of a category that was constructed during a period of mass death and social panic. The biology has changed. The inherited meaning has not kept pace.
What this produces, at the level of the individual self, is something that clinical psychology has begun to name but has not yet fully mapped. The chronic condition does not merely impose practical constraints. It demands constant negotiation between the self that existed before diagnosis and the self that the diagnosis insists upon. Some people describe the experience as a kind of permanent double consciousness — not in the sense W.E.B. Du Bois used it, though the structural parallel is not irrelevant — but in the sense of always perceiving oneself through the anticipated gaze of the other, always pre-processing one’s own identity through the filter of what the diagnosis will do to it in someone else’s eyes. This is not pathology. It is an entirely rational response to a social environment that has consistently confirmed the worst fears about disclosure.
The deeper trap is that the medical system, in offering identity coherence through the diagnosis — support groups organized around the condition, literature addressed to “people living with HIV,” community structures built around the shared fact — inadvertently reinforces the very capture it might otherwise resist.
The silence that healthy people require
You have learned, without anyone ever teaching you explicitly, exactly how much of your own life you are permitted to narrate out loud.
The unspoken arithmetic works like this: you may mention the diagnosis once, in a moment of sufficient trust, in a tone calibrated to signal that you do not intend to make it anyone’s recurring burden. After that initial disclosure, the expectation hardens into architecture. You are welcome to remain in the room, at the dinner table, inside the friendship — provided you do not bring it with you again. The silence asked of you is not presented as a demand. It arrives dressed as consideration. People tell you, with genuine warmth in their voices, that they do not want to reduce you to your condition. What they do not say, and perhaps do not consciously know, is that their own comfort depends on your cooperation with this arrangement.
Erving Goffman spent years mapping the social rituals by which stigmatized individuals manage what he called spoiled identity, and his 1963 work Stigma remains one of the most precise accounts of this invisible labor. What Goffman observed was that the stigmatized person becomes the primary worker in maintaining the social ease of everyone around them. The burden of discretion falls not on the person who holds the discomfort but on the person who triggers it by existing honestly. This is not a coincidence of etiquette. It is the structural logic of stigma itself: the minority carries the administrative cost of the majority’s unease.
The rationalization for this arrangement has proven remarkably durable. Silence is framed as privacy, and privacy is framed as dignity, and dignity is framed as something the person with HIV ought to want for themselves. By the time the argument completes its circle, the enforcement of silence appears to originate from inside the person being silenced. What looks like self-protection is often, on closer inspection, the internalization of a social contract written entirely by and for those who never had to sign it. When a man decides not to tell his colleagues, not to mention it at his brother’s wedding, not to let it surface even in casual conversations about health, he experiences that decision as agency. The experience is not false. But the conditions that make silence feel like the safest choice were not constructed by him.
There is something worth sitting with in the specific year 1996, when combination antiretroviral therapy transformed HIV from a near-certain death sentence into a manageable chronic condition. The medical emergency receded. What did not recede, at anything approaching the same pace, was the social temperature around the diagnosis. The pharmaceutical achievement allowed the broader culture to quietly reassign the problem — from a crisis requiring collective attention to a private matter requiring individual management. The urgency that had briefly made silence socially untenable dissolved back into the ordinary. And ordinary life, it turned out, had always preferred not to hear about this.
What the healthy majority rarely examines is the particular violence of normalized discretion — not the dramatic violence of explicit rejection, but the quieter violence of a world so structured around their comfort that the person living with HIV cannot speak naturally about their own fatigue, their medication schedule, their fear of transmission, their grief, without immediately sensing the temperature in the room shift. The shift is slight. It is plausibly deniable. It does not constitute cruelty by any standard definition. It is simply the atmosphere, and atmospheres do not apologize for themselves.
The social contract of discretion does not protect the person living with HIV from exposure. It protects everyone else from the specific discomfort of being present, without excuse or exit, inside a life that chronic illness has permanently altered — a life that was never asking for rescue, only for the ordinary room that is given without negotiation to everyone who does not carry a reason to require it.
🧬 Living with HIV: Body, Mind and Social Stigma
Living with HIV extends far beyond viral loads and medication schedules — it touches identity, intimacy, and the invisible walls society erects around those it fears. These articles explore the psychological, social, and existential dimensions that surround illness, stigma, and the long road toward reclaiming a full human life.
Protecting human dignity against the processes of social marginalization
Social marginalization operates through subtle mechanisms of exclusion that strip individuals of their dignity long before any formal rejection occurs. For people living with HIV, the processes described here — labeling, othering, and institutional neglect — resonate with painful familiarity. Understanding these dynamics is the first step toward dismantling them.
GO TO THE SELECTION: Protecting human dignity against the processes of social marginalization
The roots of social prejudice and the mechanisms of exclusion
Prejudice rarely emerges from nowhere; it is built on accumulated cultural fears, misinformation, and the human need to locate danger outside the self. The stigma surrounding HIV is a textbook case of how social prejudice crystallizes into systemic exclusion. This article traces the roots of those mechanisms with clarity and historical depth.
GO TO THE SELECTION: The roots of social prejudice and the mechanisms of exclusion
Illness as Awakening: When the Body Says Enough
When the body becomes the site of crisis, illness can paradoxically function as a threshold — a forced pause that compels a reckoning with how we have been living. For many people diagnosed with HIV, the medical event triggers a profound psychological and existential awakening. This piece explores how the body’s distress can become an unexpected invitation toward authentic life.
GO TO THE SELECTION: Illness as Awakening: When the Body Says Enough
The weight of the psychological past and the process of trauma liberation
The psychological weight of a chronic diagnosis does not dissolve with treatment; it lingers in memory, in relationships, and in the stories we tell ourselves about who we are now. Liberation from that burden requires a conscious process of revisiting the past without being imprisoned by it. This article offers a thoughtful framework for understanding trauma’s grip and the possibilities of release.
GO TO THE SELECTION: The weight of the psychological past and the process of trauma liberation
Discover Stories That Matter on Indiecinema
Independent cinema has long been the space where stories like these find their truest voice — raw, uncompromising, and deeply human. On Indiecinema you can explore films that confront illness, stigma, identity, and resilience with the courage that mainstream cinema rarely dares. Start streaming today and let independent film expand the way you see the world.
👉 EXPLORE THE CATALOG: Watch Indie Films in Streaming
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision

