The Invisible Architecture of Duty
You hand her the glass of water with both pills balanced on your palm, and she looks at you the way she sometimes looks at the window — not through you exactly, but past some version of you she is still trying to locate. You say her name. Not “Mom,” which stopped working sometime around last winter, but her actual name, the one her parents gave her, because that one still occasionally finds something in there, some corridor that hasn’t gone dark yet. She takes the pills. You watch her swallow. You write it down in the notebook you keep by the stove because you learned, three months ago, that memory cannot be trusted in this house — not hers, and, it turns out, not yours either, not when you’re running on five hours of sleep and the particular cognitive fog that descends when vigilance becomes the permanent weather of a life.

There is no word in common use for what has happened to your days. “Caregiver” is the clinical term, the one that appears on insurance forms and social services intake sheets, but it doesn’t touch the phenomenology of the thing — the way time has reorganized itself around another person’s dissolution, the way your own biography has quietly stepped to the side to make room for an endless present tense of tasks. You didn’t decide to become this. There was no morning when you sat down and chose it. It accumulated, the way water damage accumulates behind a wall: invisible, structural, and already extensive by the time anyone thinks to look.
What makes this particular kind of duty so difficult to name is that it arrives dressed as love. And it is love — that much is true and should not be qualified away. But love has historically been granted a certain narrative shape: it rises, it deepens, it transforms both people. What Alzheimer’s introduces into that shape is an asymmetry so radical that the usual frameworks stop functioning. The person being loved is simultaneously present and receding, capable of eye contact and incapable of continuity, still themselves in flashes that arrive without warning and vanish before you can settle into them. You learn to live inside those flashes. You stop expecting them to last.
The sociologist Arlie Hochschild, in her 1983 study of emotional labor, described the invisible work of managing feeling as a form of labor that goes systematically unrecognized precisely because it is performed through the medium of the self. She was writing about flight attendants, but the architecture she identified — the requirement to produce an emotional state in another person by suppressing or transforming your own — maps with uncomfortable precision onto what happens in a family caregiving relationship with a person experiencing dementia. You cannot be frightened when she is frightened, because your fear will amplify hers. You cannot be exhausted when she needs reassurance at two in the morning. You perform steadiness. You perform patience. You perform the fiction that everything is recognizable and safe, because her nervous system needs that fiction more urgently than you need the relief of dropping it.
Dementia care at home is now the statistical norm rather than the exception. The Alzheimer’s Association reported in 2023 that more than eleven million Americans provide unpaid care to someone with Alzheimer’s or another dementia, contributing an estimated eighteen billion hours of labor annually — labor that does not appear in GDP, that earns no wage, that accrues no pension credit, and that takes place almost entirely behind closed doors. Behind those doors, there is a notebook by the stove. There is a glass of water. There is a name being said out loud in the hope that it still means something to the person hearing it, and the particular quality of silence that follows when you cannot be sure whether it did.
Days Blows by in a Moment

Documentary, by Cristiana Donghi, Italy, 2022.
Ancilla is 86 years old. Two years ago, she moved in with her daughter Emanuela at the pandemic's beginning. Ancilla is slowly losing her memory. He does not remember what she had for lunch, she only remembers events from the past, perhaps only because she has been repeating them for years. Emanuela takes care of her, day after day she wakes her up, prepares her food, washes her, dresses her, and accompanies her a couple of days a week to the hospice and does physiotherapy. This is one of the few contacts with the rest of the world she has left. Ancilla has another child, Mauro, who has been living in London since he left looking for a job. She hasn’t seen him for two years. Daily routines always repeat themselves and change only with the changing seasons. The mother's memories slowly introduce us to Ancilla, her past, the life she lived and that transported her here. Melancholy moments alternate with funny ones and those where patience reaches its limits. Ancilla's sympathy brings a light, fresh breeze into the lives of those around her and allows them to see everything in a way where even the most ominous clouds are blown away momentarily by a breath of wind.
LANGUAGE: Italian
SUBTITLES: English, Spanish, French, German, Portuguese
When Love Becomes a Role No One Auditioned For
You did not decide to become a caregiver. The decision was made somewhere upstream of you, in the slow accumulation of assumptions about who in a family holds the emotional labor, who answers the phone when the doctor calls, who rearranges a life rather than a schedule. One morning the diagnosis arrived and, without a formal meeting or a spoken agreement, the role had already been assigned. You simply stepped into a shape that had been cut for you long before your mother forgot your name.
Arlie Hochschild’s work on the “second shift,” published in 1989, documented how women in dual-income households were performing the equivalent of an extra month of full-time work each year compared to their male partners — invisible labor that was not counted as labor precisely because it looked like love. What Alzheimer’s does to a family is essentially an acceleration of this pre-existing architecture. The disease does not invent the caregiving hierarchy; it reveals the one that was already there, encoded in who calls the aging parent most often, who keeps track of the medication, who knows the name of the primary care physician. When the crisis arrives, it simply follows the grooves already worn into the household.
The numbers are not subtle. According to the Alzheimer’s Association’s 2023 Facts and Figures report, approximately 83 percent of the help provided to older adults in the United States comes from family members, friends, or other unpaid caregivers, and of that group, roughly two-thirds are women. More specifically, daughters are the single largest category of dementia caregiver. Not spouses, not sons, not professional aides — daughters. This is not sentiment. This is infrastructure, organized along the fault lines of gender and quietly sustained by cultural narratives that frame a woman’s attentiveness as personality rather than conscription.
Sociologist Emily Abel, in her 1991 study “Who Cares for the Elderly?”, traced how the ideology of familial care in the United States was built on a Victorian foundation that treated women’s domestic labor as an expression of their inherent moral nature. The practical consequence of that ideology, more than a century later, is that when a seventy-eight-year-old man with advancing dementia needs someone to bathe him, the question of who will do it is rarely experienced as a question at all. The answer arrives pre-formed. And the person who performs that care frequently describes it not as a sacrifice but as something she simply had to do — a formulation that makes structural coercion indistinguishable from personal virtue.
There is also a class dimension that rarely surfaces in the public conversation about caregiving. Families with financial resources can hire professional home health aides, transition a parent into memory care facilities, and distribute the weight of the disease across paid labor. The families who cannot absorb those costs — and in 2023, the median annual cost of a private room in a memory care unit in the United States exceeded ninety-six thousand dollars — are left to reorganize themselves around the gap. Someone reduces working hours. Someone declines a promotion. Someone moves back into a childhood home. These adjustments are experienced as private decisions, as expressions of love, as the natural response to an impossible situation. They are rarely named as what they also are: an economic transfer, from the family to the state and the healthcare market, paid in time rather than money, and overwhelmingly drawn from women’s accounts.
What makes this particular form of structural pressure so durable is that it arrives dressed in the language of relationship. The daughter who leaves her job to care for her father with Alzheimer’s is not called exploited. She is called devoted. The vocabulary of virtue does enormous work here, sealing the arrangement from the kind of scrutiny that any other form of unpaid, mandatory labor would immediately attract.
The Medicalization of Grief
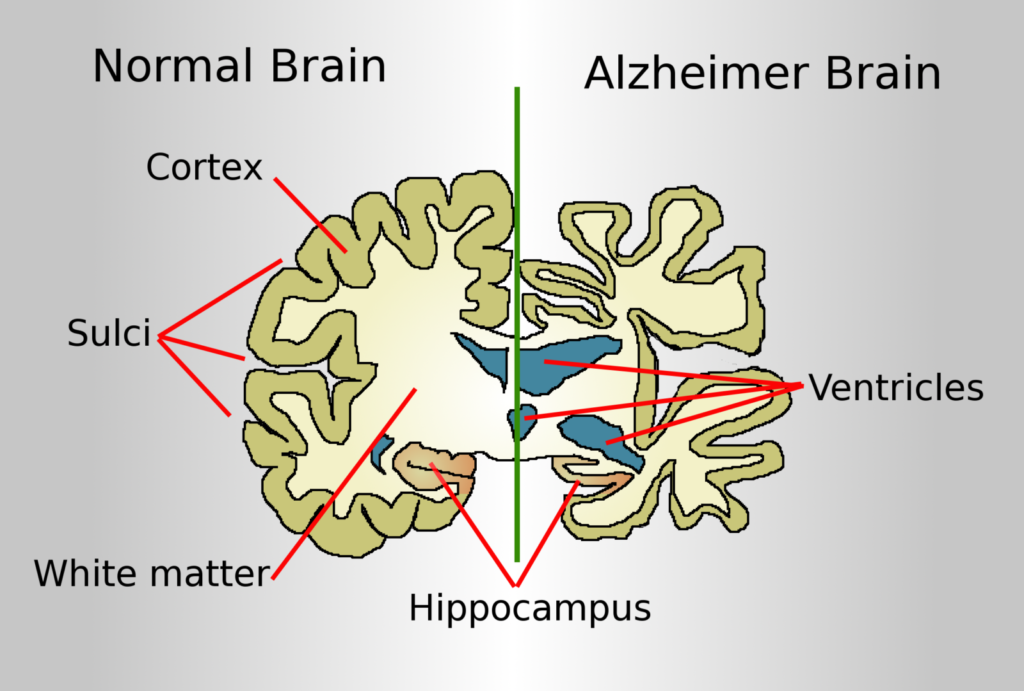
You are handed a diagnosis and told, implicitly, how to feel about it. The neurologist uses careful language, speaks of progressive cognitive decline, of plaques and tangles visible on imaging, of a timeline that cannot be reversed. You nod. You take the pamphlet. And somewhere between the parking lot and the drive home, grief becomes a clinical category, something to be managed rather than lived. This is not an accident of bedside manner. It is the long consequence of a specific historical decision made, in stages, over nearly a century.
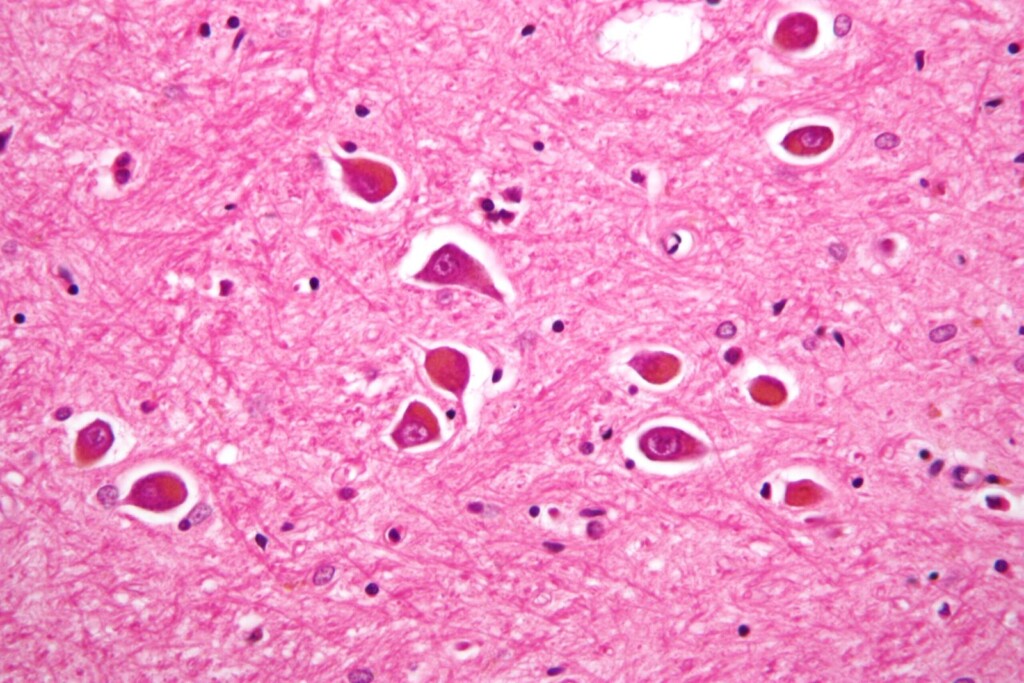
Alois Alzheimer presented his case to a gathering of German psychiatrists in November 1906 — Auguste Deter, a woman in her fifties who had lost language, memory, and finally recognition of her own husband. He described unusual cortical lesions, neurofibrillary tangles, what he called a peculiar severe disease process. His colleagues received the report with indifference. Emil Kraepelin, the dominant taxonomist of psychiatric illness at the time, later named the condition after Alzheimer in his 1910 Handbook of Psychiatry — a political gesture as much as a scientific one, consolidating his own school’s prestige by attaching names to newly delineated pathologies. For the next six decades, what we now call Alzheimer’s disease remained a marginal curiosity, applied only to patients under sixty-five. Everyone else who lost their minds in old age was simply described as senile, their deterioration considered a natural extension of aging, not a disease requiring response.
The reclassification arrived with remarkable speed in the late 1970s. In 1976, neurologist Robert Katzman published an editorial in the Archives of Neurology arguing that senile dementia and Alzheimer’s disease were biologically identical and should be merged under a single label. His argument was partly scientific, partly strategic: by combining populations, he could demonstrate a scale of suffering large enough to demand federal funding. By 1980, the National Institute on Aging had adopted this framework, and the newly formed Alzheimer’s Association began the work of transforming a pathological category into a public identity. What had been called senility — a word that carried moral weight, suggesting a kind of earned diminishment — became instead a disease with a name, a logo, a ribbon, and eventually a walk.
Naming is never neutral. When Susan Sontag wrote in Illness as Metaphor in 1978 that every disease acquires a meaning beyond its biology, she was describing how diagnosis functions as a social contract, redistributing guilt, obligation, and expectation among everyone involved. The moment a condition is named and classified, families are no longer simply witnessing someone they love become someone they struggle to recognize. They are now caregivers, a word that arrived in the American policy lexicon precisely in this same late-1970s period, carrying with it an entire architecture of duty. The word does not describe a relationship. It describes a role, and roles come with performance standards.
What gets quietly buried inside this medicalization is the grief that refuses clinical containment. Families routinely describe mourning someone who is still alive — the particular vertigo of sitting across from a person whose body continues while the familiar self has departed. Pauline Boss, the family therapist who introduced the concept of ambiguous loss in her 1999 book of the same name, spent years documenting how this unresolvable grief damages people precisely because it finds no legitimate social space. There are no funerals for the living. There are no condolence cards for the slow erosion of a personality. The medicalization of the condition creates the paradox: it raises the visibility of the disease while simultaneously rendering its emotional reality unspeakable, because grief implies loss, and loss implies an ending, and the person is still there at the table, still eating, still breathing, still occasionally saying your name in a voice that sounds exactly like the one you have loved for decades.
The Self That Stays and the Self That Dissolves
You set a photograph on the kitchen table one morning — not for them, but for yourself — and for a moment you see it too, the person who used to live behind those eyes, and you have to look away because the face across from you is wearing the same bones and the same skin and is asking you, with complete sincerity, who you are.
The question of what persists through time in a human being is not new to philosophy, but Alzheimer’s disease makes it anatomical. Derek Parfit spent the better part of the 1980s arguing, in Reasons and Persons, that personal identity is not what matters — that what we call the self is nothing more than a series of overlapping psychological connections, memories linking to intentions linking to beliefs linking to future plans, and that when those connections weaken or vanish, there is no hidden soul-substance left holding the entity together. He meant this as a liberation, a way of dissolving the ego’s grip on moral reasoning. What he could not have fully anticipated is that families living with a person whose connections have been severed would encounter his argument not as philosophy but as Tuesday afternoon.
Psychological continuity theory, which Parfit drew from and sharpened, holds that you are the same person as your ten-year-old self not because of any fixed essence but because there is an unbroken chain of memory, personality, and intention connecting you across time. Break enough of those links and the chain does not simply become shorter — it becomes a different chain entirely. This is not metaphor when a woman who spent forty years as a schoolteacher can no longer recognize her own handwriting, when a man who built furniture by hand asks what tools are for. The professional self, the relational self, the self constituted by preferences and irritations and inside jokes and grudges held and released — these are not decorations on top of a person. For Parfit, they are the person, and their disappearance is not a concealment but an erasure.
Caregivers rarely frame their grief in these terms, but they live inside the problem with a precision that no seminar can replicate. The particular cruelty is that the body continues — it breathes, it reaches, it sometimes laughs at the right moment by accident — and so the social obligation to treat it as the same person it once was remains intact and in fact intensifies, while the experiential reality of who that person was recedes past the point of retrieval. You are not mourning a death. You are mourning a continuity, which is a stranger and more disorienting form of loss because it has no ceremony, no moment of before and after, only an accumulation of absences that only you seem authorized to count.
The philosopher Christine Korsgaard, pushing back against Parfit from a Kantian direction, argued that what makes a self is not the chain of memories but the capacity to reflectively endorse one’s own identity — to author oneself over time. What happens, then, when that authorship becomes impossible, when the person can no longer ratify or refuse the story being told about them? The caregiver becomes, by default, the sole narrator. They decide what counts as a good day. They decide which version of the person before them to address — the one from thirty years ago or the one who appeared last week. They carry the full interpretive weight of another human being’s existence, and there is no handbook for what that does to a person who is also, quietly, trying to remain themselves.
There is a photograph on the kitchen table, and in it, two people are laughing at something that no longer exists in any retrievable mind, and one of those people is standing right there, close enough to touch, and the distance between them is not measured in years or miles but in the strange, specific unit of everything that cannot be remembered.
Institutions and the Guilt Architecture
You sign the admission papers on a Tuesday afternoon and drive home alone, and the silence in the car is not peaceful — it is the silence of a verdict you rendered against yourself, one that will replay without invitation for months.
That feeling did not arrive from nowhere. It was engineered. Western cultures, particularly those shaped by Christian frameworks of sacrifice and filial duty, have spent centuries constructing the moral architecture of care around proximity — the idea that love is measured in physical presence, in sleeplessness, in the willingness to absorb another person’s dissolution into your own body and schedule. When the historian Philippe Ariès traced the evolution of death and dying in his 1977 work “The Hour of Our Death,” he documented how the medicalization of dying had already begun transferring intimate processes out of the home and into institutions — and how that transfer produced not relief, but shame. The shame was not incidental. It was structurally useful.
The economics of unpaid domestic labor in care contexts are staggering in ways that rarely reach public conversation in their full dimension. In the United States alone, the AARP Public Policy Institute estimated in 2023 that family caregivers provide approximately 36 billion hours of unpaid care annually, with an economic value exceeding 600 billion dollars. Healthcare systems are not indifferent to this figure — they depend on it. Every family that internalizes the moral imperative to keep a person with Alzheimer’s at home rather than transfer them to a facility is a family that absorbs costs that would otherwise fall on public budgets or insurance structures. The guilt is not a side effect of the system. It is one of the system’s primary operating mechanisms.
The sociologist Arlie Hochschild, writing in “The Second Shift” in 1989 and later in “The Managed Heart,” made visible how emotional labor is distributed unequally across gender lines and how that distribution is naturalized through cultural scripts about who is inherently suited to care work. The person who signs those admission papers is, statistically, overwhelmingly likely to be a woman — a daughter, a daughter-in-law, a wife — who has already spent years as the primary unpaid caregiver and who now faces a secondary wave of social judgment for the decision to delegate. The guilt architecture is gendered not by accident but by design, because the alternative — paying fairly for the labor that sustains the entire informal care economy — would require a political reckoning that no government in the developed world has yet been willing to have.
Care facilities themselves exist along an extraordinary spectrum that the language of moral failure completely obscures. A well-staffed memory care unit can offer a person with moderate-to-severe Alzheimer’s something a family home structurally cannot: round-the-clock specialized supervision, sensory environments calibrated to reduce agitation, consistent routines maintained by staff trained specifically in dementia progression. The decision to place someone in such a facility is not an abandonment of care — it is sometimes the most precise and demanding act of care available, precisely because it requires overriding your own emotional need to remain indispensable.
What keeps the guilt mechanism operational is the conflation of presence with quality. A family member who visits three times per week, who knows the person’s history and speaks their name with genuine recognition, who advocates fiercely within a professional care environment, is providing something irreplaceable — but it is not the same thing as being the full-time unpaid body in the room. The distinction matters because collapsing it allows an entire political economy of invisible labor to continue operating beneath the threshold of policy debate, funded by the private suffering of people who believe they are simply failing to love correctly.
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision
The Second Body: Caregiver Deterioration as Statistic

You wake up one morning and realize you cannot remember the last time you slept past five. Not because of an alarm, but because the body has stopped trusting silence — it listens even in unconsciousness, calibrated to the sound of shuffling feet, a cry, something falling in the hallway. You are not sick. No physician has your name on a chart. You do not exist, clinically speaking, as someone who needs watching.
And yet the data are unambiguous and have been for decades. Janice Kiecolt-Glaser at Ohio State University, working through the 1980s and into the 1990s with her colleague Ronald Glaser, drew blood from family caregivers of Alzheimer’s patients and found something that should have restructured public health policy and never quite did: the immune systems of these caregivers were measurably compromised. Their wounds healed more slowly — in one landmark 1995 study published in The Lancet, dermal punctures in caregiver subjects took an average of nine days longer to close than in matched controls. Nine days. The body’s capacity to defend and repair itself, quietly eroding in someone who has never been given a diagnosis, never been offered a treatment plan, never been told by any institution that what is happening to them constitutes a medical event.
The mortality figures sharpen this into something almost unbearable to look at directly. Research published in JAMA in 1999 by Richard Schulz and Scott Beach, tracking 392 caregiving couples over four years, found that caregivers who reported experiencing strain had a mortality risk 63 percent higher than non-caregiving controls of the same age. Not higher rates of exhaustion. Not higher rates of reported unhappiness. A 63 percent increase in the likelihood of dying. Caregiving, under conditions of sustained psychological stress without adequate support, kills the person providing care at a rate that would trigger emergency intervention if it were a pathogen, a workplace toxin, an environmental contaminant.
Depression prevalence among Alzheimer’s caregivers hovers between 30 and 40 percent depending on the population studied — a figure roughly three to four times the general population rate. But depression in this context rarely presents as the depression that clinical culture has learned to recognize and treat. It arrives instead as flatness, as the gradual disappearance of a life that used to exist around the edges of responsibility. Friendships not ended but simply unfed until they stop. A body that moves through the day competently and feels nothing doing it. The Diagnostic and Statistical Manual has language for this, but the infrastructure to act on that language, when the sufferer is defined primarily by their relation to someone else’s diagnosis, is largely absent.
What the epidemiology reveals is the existence of a second patient — one that the medical system has structurally decided not to see, because seeing them would require acknowledging that the labor sustaining an Alzheimer’s patient at home is not free, not neutral, not without consequence. The Alzheimer’s Association estimated in its 2023 Facts and Figures report that American caregivers of people with dementia provided 18.4 billion hours of unpaid care in the preceding year. Eighteen billion hours of biological cost, immunological cost, neurological cost, absorbed entirely by private individuals who are never screened, never monitored, and never compensated for the physiological damage accumulating in their own tissue while they manage someone else’s.
There is a particular cruelty embedded in the cultural script that frames this arrangement as love. Love it may be, and often is — but the framing serves a function that has nothing to do with love, which is to make the transfer of catastrophic biological burden from the state to the family appear voluntary, natural, and therefore invisible to any accounting that might demand redress. The body of the caregiver deteriorates inside a story that celebrates its deterioration as devotion, and medicine, largely, has not interrupted that story.
Time Colonized
She is sitting in a meeting that has been going on for forty minutes, and she has understood perhaps three consecutive sentences of it. Her body occupies the chair with reasonable conviction. Her eyes track the speaker. But the actual architecture of her attention is somewhere on the other side of the city, running a parallel calculation: her father’s home aide arrives at nine, leaves at two, and there is a window between two and four when he is alone, and yesterday he left the gas on, and she has not yet called the neighbor with the spare key, and she needs to call before noon because the neighbor leaves for her own appointments at noon, and it is currently eleven forty-seven, and the meeting shows no sign of ending, and the slide on the screen says something about Q3 projections, and she nods.
This is what cognitive science would call a “split attention cost,” but that phrase makes the phenomenon sound manageable, like a bill you pay in installments. What it actually describes is closer to what the neurologist and trauma theorist Bessel van der Kolk documented in his research on intrusive thought patterns — the way a mind under chronic threat cannot fully inhabit any present moment because some portion of its processing capacity has been permanently reassigned to monitoring, to threat-scanning, to the running maintenance of a situation that refuses to resolve. Van der Kolk was writing about post-traumatic stress, but the structural mechanics are nearly identical: a nervous system that has learned the present is never safe enough to fully occupy.
Sociologist Arlie Hochschild introduced the term “emotional labor” in 1983 to describe the invisible work of managing feelings as a professional requirement, but she was describing something that remained, at least in theory, bounded by a shift, a workplace, a contract. What dementia care produces is something without those limits — not emotional labor but emotional tenancy, where the condition takes up permanent residence inside the caregiver’s cognitive life and pays nothing in return. Studies published in the journal Gerontologist have found that family caregivers of dementia patients report spending an average of forty-seven hours per week in direct or indirect caregiving activity, a figure that effectively renders caregiving a second full-time occupation — one with no salary, no benefits, and no clocking out.
The insidious feature of this colonization is that it operates invisibly even to the caregiver. Time does not feel stolen because there is no discrete moment of theft. There is only the gradual discovery that the mental bandwidth once available for reading, for desire, for sustained curiosity about anything unrelated to medications and incontinence schedules and insurance reimbursements, has been quietly redistributed. Psychologist Christina Maslach, whose foundational research on burnout from the 1970s onward established that exhaustion is not primarily physical but the result of chronic emotional depletion, identified depersonalization as one of its core symptoms — a flattening, a going-through-of-motions, a suspension of the self that once existed before the demands arrived. Caregivers describe this in almost identical language: not unhappiness exactly, but a kind of temporal amnesia, an inability to locate who they were before this became their life.
What makes this particularly difficult to name is that the culture surrounding caregiving actively suppresses its naming. The dominant moral vocabulary insists that love expressed through sacrifice is its own reward, which is a way of saying that those who lose the most should feel grateful for the opportunity. Time surrendered to care is framed as time given freely, which forecloses any honest accounting of what the surrender actually costs — and what it costs is not just hours but the particular texture of a life that had other intentions, other directions, other possibilities it was quietly moving toward before the diagnosis arrived and rerouted everything without asking.
The Question the Family Never Gets to Ask
You find yourself holding a legal document your mother signed eleven years ago, in a kitchen that smelled like coffee and certainty, and the words on the page no longer match the person sitting across from you — not because the document was wrong, but because no document written by a self that still existed could ever fully authorize decisions made for a self that has since become someone else.
This is the fracture at the center of every Alzheimer’s care arrangement, and it is one that bioethics has circled without ever fully entering. The concept of advance directives, formalized in the United States through the Patient Self-Determination Act of 1990, was built on a philosophically generous assumption: that a competent self could speak reliably on behalf of a future incompetent one. But Ronald Dworkin, in his 1993 work Life’s Dominion, already identified the tension that legal frameworks preferred to suppress — that the person who made the directive and the person now living inside the disease may not share the same interests, the same fears, or even the same relationship to suffering. What the earlier self feared most may be precisely what the later self has adapted to. The family is then left not executing a wish but interpreting a ghost.
What makes this silence particularly heavy is that medicine has grown technically capable far faster than it has grown morally precise. The average person living with Alzheimer’s today survives between eight and twelve years after diagnosis, according to data from the Alzheimer’s Association, which means that families do not face a single decisive moment of crisis but rather thousands of incremental choices distributed across a decade — choices about nutrition, about restraint, about whether a small deception is kinder than a painful truth, about whether keeping someone alive in a state of total dependence honors their dignity or quietly violates it. No directive written in a kitchen covers all of this.
The weight falls on whoever is closest, and closeness here is rarely chosen with full knowledge of its consequences. A 2019 analysis published in Health Affairs found that over 75 percent of dementia caregivers in the United States are family members, and that the average family caregiver provides more than 47 hours of care per week — figures that describe not a role but an absorption. The person giving care does not simply help; they gradually become the external architecture of another person’s existence, making decisions that were never theirs to make by any design anyone would have consciously endorsed.
What language has failed to name is the specific ethical position of someone who loves the patient enough to act and knows the patient well enough to doubt whether any action is truly right. It is not guardianship in the legal sense, not medical proxy in the clinical sense, not grief in the psychological sense — it is something anterior to all three, a kind of compelled authorship over a life that still belongs to someone else. The philosopher Agata Cieślak, writing on relational autonomy in care contexts, has argued that autonomy is never purely individual but always constituted through relationships — which means that when the patient can no longer exercise it, the relational network does not lose it but inherits it in a form no one agreed to receive.
And so the family carries a question that has no clean answer and no sanctioned place to ask it aloud: not whether they love the person, which is rarely in doubt, but whether the arrangement they are sustaining is one that person would recognize as belonging to their life — or whether it is something the living do for themselves, in the name of someone who has already moved beyond the reach of names.
🧩 When Care Becomes a Labyrinth of Love
Alzheimer’s does not only transform the person who lives with it — it reshapes the entire family around them. These articles explore the psychological, emotional, and cultural landscapes that surround dementia, caregiving, and the slow grief of losing someone who is still present.
Senile Dementia: the Lost Memory
Senile dementia strikes at the very core of personal identity, eroding the memories that make us who we are. This article traces the medical and human history of a condition that forces families to confront the gradual disappearance of a loved one. Understanding its nature is the first step toward navigating the daily reality of care with greater compassion.
GO TO THE SELECTION: Senile Dementia: the Lost Memory
The Family Caregiver: Psychology and Culture of Care
The family caregiver occupies a unique and often invisible role in contemporary society, balancing love, exhaustion, and duty in ways that rarely receive public recognition. This article examines the psychological toll and cultural meanings of care, exploring how different societies value — or neglect — those who dedicate their lives to another. It is essential reading for anyone living inside the demanding world of daily caregiving.
GO TO THE SELECTION: The Family Caregiver: Psychology and Culture of Care
Anticipatory Grief: When We Lose Someone Still Alive
Anticipatory grief is the profound mourning we experience when someone we love is still physically present but has already begun to fade from us. This article explores a form of loss that is particularly acute in Alzheimer’s families, where the farewell is not a single moment but a long, slow dissolving. Naming this grief is itself an act of care, both for the caregiver and the person they tend.
GO TO THE SELECTION: Anticipatory Grief: When We Lose Someone Still Alive
The Pandemic and the Elderly: Isolation and Loneliness
The pandemic cast a harsh light on the vulnerability of elderly people and their families, amplifying isolation and loneliness at a time when human connection was already strained. This article examines how social distancing deepened the suffering of those living with dementia and those caring for them, often in silence and without support. The lessons of that period remain urgently relevant for anyone thinking about aging, family, and care.
GO TO THE SELECTION: The Pandemic and the Elderly: Isolation and Loneliness
Discover the Human Stories That Cinema Doesn't Always Tell
On Indiecinema you will find independent films that dare to look closely at life as it really is — stories of illness, love, family, and resilience told without filters. Explore our streaming catalog and let cinema accompany you through the most human of journeys.
👉 EXPLORE THE CATALOG: Watch Indie Films in Streaming
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision

