The Intimacy Paradox
You have been with this person for four years. You know the sound they make when they are almost asleep, the exact weight of their arm across your chest, the particular silence that means they are thinking about something they will not say until morning. You have shared fevers and funerals and the specific exhaustion that comes from loving someone through a hard season. And somewhere inside all of that accumulated knowledge, inside the architecture of that intimacy, a quiet assumption has been building without your permission: that closeness itself is a form of protection.

It is not. And the history of HIV transmission inside long-term partnerships is, in large part, the history of that assumption being proven catastrophically wrong.
The epidemiological record is unambiguous on this point, even when the cultural narrative refuses to absorb it. The CDC’s own surveillance data has demonstrated for decades that a substantial proportion of new HIV infections in the United States do not occur between strangers or in the transactional, anonymous encounters that dominate the public imagination of the epidemic. They occur between people who share a home, a surname, a savings account, a decade. A 2016 analysis published in the Annals of Internal Medicine found that among HIV-negative individuals in serodiscordant relationships — partnerships where one person is living with HIV and the other is not — the perception of reduced risk was inversely correlated with consistent protective behavior. The longer the relationship, the lower the perceived threat. The lower the perceived threat, the less likely the couple was to maintain the practices that actually interrupt transmission.
What is happening psychologically in that gap between perception and reality has been examined carefully by researchers working in the tradition of cognitive dissonance theory, first formalized by Leon Festinger in his 1957 work A Theory of Cognitive Dissonance. Festinger demonstrated that human beings are not primarily truth-seeking organisms; they are consistency-seeking ones. When a belief — this person is safe, this relationship protects me — collides with a behavior that contradicts it, the mind does not typically abandon the belief. It distorts the behavior, reclassifies the risk, or simply refuses to complete the calculation. In the context of HIV, this is not a personal failure. It is a structural feature of how intimacy is taught and understood in virtually every society that produces long-term monogamous partnerships as a normative ideal.
The institution of monogamy carries an embedded promise that is rarely stated explicitly but functions with enormous force: exclusivity equals safety. This promise predates germ theory. It was doing cultural work long before anyone understood the mechanics of viral transmission, and it has proven remarkably resistant to scientific revision. When researchers from the University of Washington’s Partners in Prevention HSV/HIV Transmission Study tracked over three thousand serodiscordant heterosexual couples across seven African countries between 2004 and 2008, they found that relationship duration was one of the strongest predictors of inconsistent condom use, not because these couples were uninformed or indifferent, but because the emotional logic of a sustained partnership actively undermined the clinical logic of risk management. Love, or something that functions like it, was doing the work of suppression.
This is the intimacy paradox in its most precise form: the same relational depth that motivates people to protect each other also generates the psychological conditions under which protection is quietly abandoned. The vulnerability required to sustain long-term love — the lowering of defenses, the dissolution of vigilance, the willingness to be known completely — is neurologically and behaviorally antagonistic to the sustained alertness that effective HIV prevention requires. It is not that people in long-term relationships are careless. It is that the very thing that makes a relationship feel permanent also makes danger feel like an abstraction belonging to another kind of life, a life they believe they have already left behind.
Serodiscordant Partnerships and the Architecture of Risk
You have been with this person for three years. You know the sound of their breathing when they are almost asleep, the exact temperature they keep the shower, the way they hold their fork. You have built what the culture calls intimacy. And then one afternoon a test result arrives, and the architecture of that familiarity suddenly reveals a structural flaw that was always there, invisible, load-bearing.
Serodiscordant relationships — those in which one partner carries HIV and the other does not — are far more common than public health discourse tends to acknowledge, and their existence exposes a foundational confusion between emotional proximity and biological risk. The assumption that commitment provides some form of immunological shelter is not merely naive; it is statistically demonstrable as dangerous. Research published in the journal Lancet Infectious Diseases in 2012 analyzing data from forty-seven African countries found that a substantial proportion of new HIV infections occurred within stable, cohabiting partnerships, not through the casual encounters that dominate prevention campaigns. The number was not marginal. In some regions, it exceeded fifty percent of all new transmissions.
What that figure requires is not sympathy but precision. Viral load is the central variable, and it behaves with an indifference to sentiment that the medical literature has documented with increasing granularity since the early 1990s. A person on effective antiretroviral therapy who achieves an undetectable viral load transmits HIV at a rate that multiple large-scale studies, including the PARTNER study completed in 2019 following over one thousand serodiscordant couples across Europe, measured at effectively zero — across approximately seventy-seven thousand condomless sex acts. Zero transmissions. The biological risk does not disappear because love is present; it disappears because suppressive treatment intervenes in the mechanics of transmission itself.
This distinction matters because it relocates the danger. The threat in a serodiscordant partnership is not the relationship’s duration or depth. It is inconsistency: interrupted treatment, undisclosed status changes, the assumption that stability means stasis. A partner who was undetectable eighteen months ago and has since stopped therapy due to side effects, financial barriers, or the psychological weight of daily pharmaceutical routine represents a different viral reality than the test result from the beginning of the relationship suggested. Relationships maintain their narrative continuity while biological conditions shift beneath them, and the human capacity for wishful updating — for treating past safety as present safety — does exactly what cognitive psychologist Daniel Kahneman identified in Thinking, Fast and Slow as the substitution heuristic: replacing a question that requires hard work with a more comfortable one that feels equivalent.
There is also the question of what serodiscordancy reveals about diagnosis itself. The Centers for Disease Control and Prevention estimated in 2021 that approximately thirteen percent of Americans living with HIV remained undiagnosed. A serodiscordant couple is not always aware it is one. When transmission occurs within a committed partnership between people who believe themselves concordant, the epidemiological record registers a casual transmission in the absence of known contact — which skews both risk modeling and prevention targeting away from precisely the contexts where intervention would be most useful.
The category of the committed relationship has historically functioned as a permission structure in public health messaging — a threshold past which vigilance was implicitly relaxed. The cultural logic is comprehensible: two people building a shared life presumably reduce their external exposure, and reduced exposure reduces risk. The error lies in treating reduced as eliminated, and in failing to account for the biological independence of a virus from the emotional contracts its hosts have made with one another. HIV does not read the relationship as the people inside it do. It reads membrane permeability, viral concentration, and mucosal integrity — variables that no anniversary, no shared lease, no history of accumulated mornings can alter.
The Sociology of Trust as a Public Health Variable

You stopped using condoms not because the risk disappeared but because stopping felt like the right thing to do at that point in the relationship. There was a conversation, or perhaps there was no conversation at all — just a gradual drift toward bare skin that neither of you formally authorized, because formalizing it would have required acknowledging what you were actually deciding. The absence of discussion was itself the agreement.
Niklas Luhmann, in his 1968 work Vertrauen, made a distinction that most people in long-term relationships would find uncomfortable if they ever encountered it directly: trust, he argued, is not a form of knowledge but a substitute for it. You trust precisely because you cannot verify. The couple who stops using condoms after two years together is not acting on confirmed information about each other’s serostatus or behavioral fidelity — they are acting on a social mechanism that reduces complexity by treating the unknown as if it were known. The intimacy of the relationship does its cognitive work by generating a feeling of safety that has no epidemiological basis.
This is where the sociology becomes a clinical variable. Studies tracking seroconversion events in stable partnerships — among them the large-scale European HSV/HIV Transmission Study published across the late 1990s and early 2000s — found that a substantial proportion of new infections occurred within relationships that the infected partners themselves described as monogamous and low-risk. The subjective assessment of risk had inverted: the longer the relationship, the lower the perceived danger, even as the actual transmission window remained structurally unchanged. Duration had become a proxy for safety, not because duration provides immunity but because it accumulates social meaning that competes with and eventually displaces biological reality.
Erving Goffman’s concept of face-saving interaction offers a partial explanation for why couples rarely renegotiate prophylactic practices even when circumstances change. To raise the subject of protection again — after months or years without it — is to perform a kind of social accusation. It implies either that you suspect your partner, or that you have something to disclose yourself. The conversation is structurally loaded before a single word is spoken, which means it tends not to happen. Partners who have received an STI diagnosis, or who have reasons to doubt the exclusivity of the arrangement, report enormous difficulty reopening what feels like a closed social contract. The bedroom has its own grammar, and that grammar does not easily accommodate the vocabulary of risk management.
What makes this particularly sharp as a public health problem is that the dynamic is not specific to any population. Research conducted by Maria Xiridou and colleagues, published in AIDS in 2003, modeled HIV transmission patterns among men who have sex with men in Amsterdam and found that steady partnerships — not casual encounters — accounted for the majority of new infections in that community. The finding challenged a decade of prevention messaging that had focused almost entirely on the anonymous encounter, the one-night risk, the stranger. The architecture of sustained intimacy was generating more transmission events than the situations everyone was warned about, because sustained intimacy had been culturally coded as its own form of protection.
There is a sociological term for the process by which a practice becomes legitimate simply through repetition within a group: normative institutionalization. The couple that has not discussed HIV testing in three years has not made a series of ongoing decisions — they have made one decision once and then allowed it to harden into invisible infrastructure. Anthony Giddens, writing in The Transformation of Intimacy in 1992, described how modern relationships are structured around what he called the pure relationship — a bond sustained only by mutual satisfaction and free in principle from external obligation. What he did not fully reckon with is how that freedom generates its own coercions, its own unspoken rules about which conversations are permitted and which ones corrode the fabric of what has been built.
Undetectable Equals Untransmittable: Science Versus Cultural Lag
You have probably never told your partner the exact number. The viral load result sitting in your clinic file — a number that determines, with near-absolute scientific certainty, whether transmission between you is biologically possible — remains unspoken, tucked behind the administrative language of “undetectable,” a word that itself gets swallowed by the far louder cultural noise insisting that HIV is always, perpetually, a weapon someone carries.
The science arrived with unusual precision. Between 2010 and 2017, the PARTNER study followed 888 serodifferent couples — one partner HIV-positive, one HIV-negative — through approximately 58,000 condomless sexual acts. The HIV-positive partners were on antiretroviral therapy and maintaining undetectable viral loads. The result: zero linked transmissions. Not a reduction. Not a negligible rate. Zero. Opposites Attract, a parallel study conducted across Australia, Thailand, and Brazil and published in The Lancet in 2017, confirmed this finding across gay male couples with the same structural rigor. The scientific community responded by formalizing a consensus: when viral load is suppressed below detectable thresholds, sexual transmission does not occur. The framework was named U=U — Undetectable Equals Untransmittable — and endorsed by the Centers for Disease Control, the World Health Organization, and virtually every major HIV clinical body on earth.
What medicine ratified in 2017, culture has largely refused to absorb. This is not simply a matter of public ignorance waiting to be corrected by better information campaigns. Cultural beliefs about disease, risk, and moral contamination do not update the way clinical guidelines do. They accumulate across decades, calcify into instinct, and resist revision precisely because they are not held as beliefs at all — they are held as obvious facts, the kind that feel too self-evident to examine. Susan Sontag identified this mechanism in Illness as Metaphor as early as 1978, arguing that serious diseases inevitably attract narrative layers that exceed their biological reality, transforming medical conditions into moral verdicts. HIV attracted more of those layers faster than almost any disease in modern history, and the metaphors have outlasted the medicine.
Inside long-term relationships, this cultural lag does not produce abstract confusion. It produces specific, recurring damage. The HIV-positive partner who knows their viral load is undetectable still navigates a partner who flinches, still absorbs the residual anxiety that scientific reassurance cannot fully dissolve, still internalizes the possibility that their body is understood as permanently dangerous regardless of what the laboratory says. The HIV-negative partner, meanwhile, may be managing not ignorance but something more stubborn: a fear that learned itself before the evidence existed and has no real mechanism for unlearning. These are not symmetrical problems. One person carries the weight of being the potential vector; the other carries the weight of managing risk they have been culturally trained to perceive as existential. Neither the weight nor the asymmetry disappears because a study published in a medical journal declared them unnecessary.
There is also a legal dimension that makes the cultural lag actively coercive. In dozens of jurisdictions, HIV non-disclosure laws were written before U=U existed as a scientific framework, and many have not been revised to account for it. A person with an undetectable viral load, in a long-term relationship, engaging in acts that carry zero transmission risk by the most rigorous available evidence, may still face criminal exposure for non-disclosure depending on where they live. The law, in these cases, is not regulating actual risk. It is enforcing a cultural narrative about contamination that the science has already dismantled, punishing people not for what they have done biologically but for what they represent symbolically.
What this means for intimacy is that two people can be in a relationship where one of them is not actually at risk, both of them know this intellectually, and the knowledge still fails to reach the register where fear, desire, and closeness live.
Gender, Power, and the Negotiation of Disclosure
You already know how this conversation ends before it starts. You are sitting across from someone you have shared a bed with for three years, and the words are fully formed in your throat, and you swallow them again, because the calculus of what comes next is not medical — it is architectural. It involves who owns the lease, who controls the car, whether the children sleep in this house or another one by the end of the month. Disclosure is never simply a health decision. It is a negotiation conducted entirely within a pre-existing structure of power, and for a significant portion of people living with HIV in long-term partnerships, that structure is violently skewed before the conversation even begins.
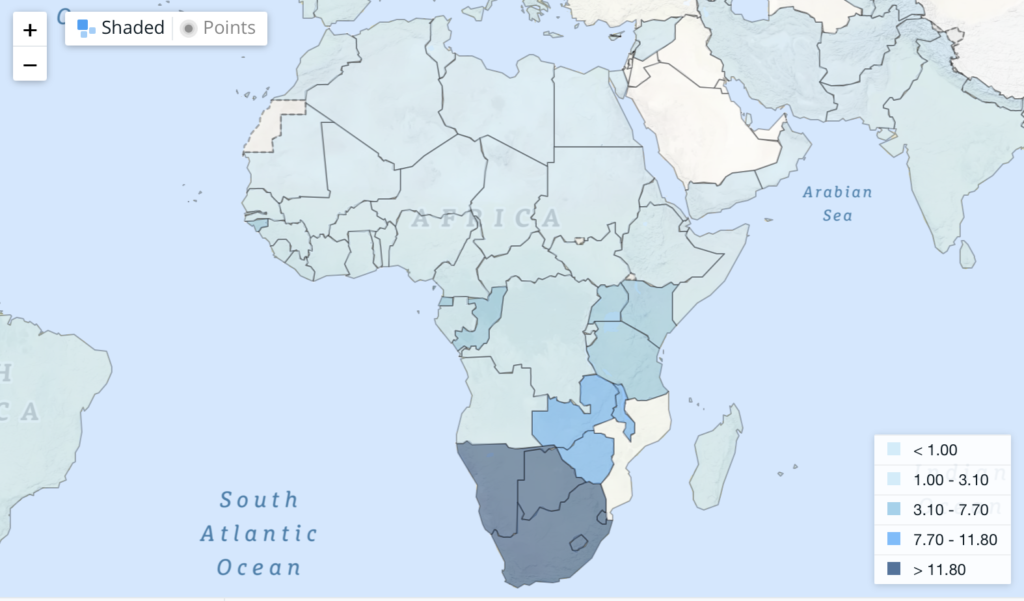
Feminist public health scholarship has spent decades documenting what clinical HIV guidelines consistently underweight: that the formal imperative to disclose — encoded in laws across more than thirty American states and numerous countries in the Global South — lands differently depending on which body carries it. Women account for roughly 53 percent of people living with HIV globally according to UNAIDS data from 2022, and in sub-Saharan Africa that figure reaches approximately 63 percent. The overwhelming majority of these women acquired the virus within stable, long-term, often formally recognized partnerships. What the epidemiological record captures as a transmission statistic, the sociological record captures as a narrative of constrained agency: women who knew their status and could not speak it, not because they lacked information, but because disclosure carried the documented risk of physical violence, economic abandonment, or social exile. Dworkin, Heise, and Lippman, writing across the 2000s and 2010s in journals including Social Science and Medicine, built an evidentiary base showing that fear of intimate partner violence is among the strongest predictors of non-disclosure among women in serodiscordant relationships — stronger, in many documented cohorts, than viral load anxiety or transmission guilt.
The man who does not disclose operates inside a different architecture entirely. His silence is more frequently scaffolded by shame and the particular social contract of masculine invulnerability — the cultural instruction that illness is a form of failure and that admitting it collapses status. This is not innocence, but it is a distinct mechanism. The sociologist Raewyn Connell, whose work on hegemonic masculinity reshaped gender studies from the 1990s onward, identified how dominant frameworks of manhood punish precisely the vulnerability that honest disclosure requires. When a man living with HIV in a long-term relationship withholds his status, he is often simultaneously protecting an image of himself that the relationship itself was built to confirm. The partner does not just lose medical information. She loses access to a self that was never fully offered.
What makes this particularly disorienting is that the public health apparatus designed to address it so frequently misreads the room. Couples counseling interventions, however well-intentioned, tend to assume a baseline symmetry — that both partners arrive at the table with roughly equivalent capacity to speak, refuse, or leave. The evidence suggests otherwise. A 2016 analysis published in AIDS and Behavior examining disclosure outcomes across multiple low- and middle-income countries found that women in relationships where their male partner held primary economic control were significantly less likely to disclose their own positive status, and significantly more likely to have their partner’s undisclosed status remain unknown to them until a later clinical event. The intervention imagines two equal speakers. The bedroom contains a landlord and a tenant.
This is where the legal framework compounds the injury rather than relieving it. Criminalization of non-disclosure does not distribute its consequences evenly. It falls with measurable disproportionality on women, on Black and brown communities, on those whose poverty makes legal defense structurally inaccessible — a pattern documented exhaustively by the Canadian HIV/AIDS Legal Network through the 2010s. The law frames silence as moral failure while the conditions producing that silence remain entirely unaddressed.
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision
PrEP, Monogamy, and the Politics of Prevention

You find out your partner has been quietly taking a daily pill, and something in you shifts before you even know what the pill is. The information arrives as betrayal before it arrives as medicine.
PrEP — pre-exposure prophylaxis, specifically tenofovir disoproxil fumarate combined with emtricitabine, approved by the FDA in 2012 under the name Truvada — reduces the risk of HIV transmission through sexual contact by approximately 99 percent when taken consistently. It is, by any clinical measure, one of the more remarkable biomedical achievements in the history of infectious disease prevention. And yet its adoption inside committed long-term relationships remains stubbornly low, not because of ignorance about its efficacy, but because of what it socially signals. A 2019 study published in AIDS and Behavior found that among serodiscordant and seroconcordant couples, a significant barrier to PrEP uptake was not side-effect profiles or cost alone, but the partner’s perceived reaction — the anticipatory fear of what the pill would communicate about trust, about loyalty, about what the person taking it privately believed was happening in the relationship.
This is the point where ideology hardens into something physiologically dangerous. Monogamy, as a cultural institution in the Western world, traces its moral architecture at least partly to Augustine of Hippo, whose Confessions constructed sexual exclusivity as the antidote to the restlessness of desire, the body brought to heel by covenant. What Augustine built as theology, later centuries converted into social contract, and what social contract became in the twentieth century was a form of identity verification. To claim monogamy is to claim a certain kind of person — trustworthy, controlled, legible. PrEP, in this economy of meaning, reads as a quiet admission that the claim is false, that someone in the partnership is not fully legible, that the contract has a clause the other person doesn’t know about.
The sociologist Anthony Giddens, writing in The Transformation of Intimacy in 1992, argued that what he called the “pure relationship” — the modern ideal of a partnership based entirely on mutual emotional satisfaction rather than economic or reproductive necessity — demands continuous acts of trust precisely because it lacks the external scaffolding of older arrangements. There is nothing holding two people together except the daily choice to remain. This makes trust both the central currency and the most precarious one. PrEP doesn’t threaten a pure relationship from outside; it threatens it from inside the logic of trust itself, because it implies that one partner is managing risk rather than simply believing. And belief, in the pure relationship, is supposed to be enough.
What gets obscured in this dynamic is the epidemiological reality that long-term partnerships account for a substantial proportion of new HIV transmissions globally, not because people are lying at rates higher than they ever were, but because the structural assumption of zero risk inside commitment creates exactly the conditions where testing lapses, conversations don’t happen, and a single event outside the relationship — a business trip, a period of distance, a night that neither person knows how to talk about afterward — passes silently into shared biology. The monogamy that exists as practice is statistically never identical to the monogamy that exists as declaration.
What makes this genuinely difficult to think about is that the resistance to PrEP inside relationships is not irrational by the logic of the system it operates within. If your relationship’s coherence depends on mutual belief rather than mutual verification, then verification is a form of aggression. The pill does not just protect the body — it introduces an epistemology. It says: I know that certainty is not the same as safety. And for a great many people, inside the architecture of what committed love is supposed to mean, that sentence is not a medical insight.
The Historical Sediment of Stigma Inside the Couple
You are sitting across from the person you have shared a bed with for eleven years, and the doctor has just used the word “positive,” and before a single conscious thought forms, something older and uglier than your relationship moves through the room. It is not grief. It is not fear. It is accusation, and it arrives before either of you has spoken.
That reflex does not belong to you personally. It was installed decades before you met, during a period when public health institutions, religious authorities, and mainstream media collaborated — not conspiratorially, but structurally — to fuse a viral transmission pathway with a moral verdict. The CDC’s earliest surveillance reports from 1981 used the term “risk groups” rather than “risk behaviors,” a categorization that embedded identity rather than action as the site of danger. By 1983, the framework was already calcified: certain people were the disease, not carriers of it. That distinction, seemingly technical, determined how an entire generation learned to feel about infection, and those feelings did not retire when the science corrected itself.
Erving Goffman, writing in Stigma in 1963, described how discredited identities function as “spoiled” ones — not merely disadvantaged, but ontologically contaminated, requiring the stigmatized person to manage the gap between who they are and who they are presumed to be. What the AIDS crisis accomplished was to industrialize this process, to give it prime-time distribution. Susan Sontag tracked this operation explicitly in AIDS and Its Metaphors in 1989, demonstrating how the language of plague had always served as a technology for moral sorting — and that HIV became its most efficient modern instrument. The consequence she could not fully anticipate was how thoroughly that sorting would migrate inward, becoming the grammar of self-interpretation for people who contracted the virus and for those who loved them.
Inside long-term relationships, this internalized grammar functions as a secondary immune disorder. A diagnosis does not arrive as a neutral medical fact to be processed together. It arrives pre-loaded with decades of cultural software that reads transmission as evidence of transgression. Partners who have been faithful, careful, and devoted find themselves auditing their own histories with prosecutorial intensity, not because the evidence demands it, but because the inherited framework demands a culprit. The relationship becomes a crime scene before it has the chance to become a medical situation.
What makes this particularly resistant to correction is that the moral frameworks of the 1980s and 1990s were never formally retracted. They were not publicly dismantled the way a law might be repealed or a scientific paper retracted. They simply became unfashionable, retreating from explicit discourse while remaining fully operational in the emotional architecture of anyone who was shaped by that period — which includes people who were children then, absorbing the ambient atmosphere of contamination and shame without the vocabulary to name what they were absorbing. A person who was eight years old in 1987 watching news coverage of AIDS deaths did not receive that information neutrally. They received it inside a moral envelope that associated the virus with deviance, with secrecy, with the consequence of transgressive desire.
By the time that person is forty and their long-term partner receives a diagnosis, the eight-year-old’s education is still running. It does not announce itself. It appears as a quality of silence in the room, as an instinct to ask certain questions rather than others, as a readiness to interpret ambiguity as evidence of betrayal. The couple believes they are responding to a medical event in the present, but they are also enacting a script written by institutions most of them would consciously reject — the televangelist, the tabloid, the senator who said the afflicted had no one to blame but themselves.
Undetectable viral loads and treatment-as-prevention protocols have transformed the clinical landscape entirely, but they operate at a different layer than the one where shame lives.
Viral Load, Time, and the Illusion of Accumulated Safety
You have been with this person for eleven years. You know the sound of their breathing when they sleep, the particular way they hold a coffee cup, the exact pitch of their laugh before it becomes genuine. And somewhere in that accumulated knowledge, without ever deciding to, you concluded that the virus does not apply to you anymore.
This is not ignorance. It is a cognitive architecture that humans build automatically when intimacy extends across time. The psychologist Daniel Kahneman, in his 2011 work on the two systems of human thought, documented how the mind substitutes difficult statistical questions with easier emotional ones. Asked how dangerous a situation is, the brain answers a different question instead: how familiar does this feel? Familiarity, after years of shared life, registers as safety. The body does not distinguish between these categories, but the mind insists on treating them as equivalent.
What makes this substitution so difficult to disrupt is that it is partially self-confirming. If nothing has happened after a decade, the nervous system reads that history as evidence of immunity rather than as a statistical run that continues forward into uncharted time. Nassim Nicholas Taleb spent much of his 2007 book on unpredictable catastrophic events explaining how organisms and institutions systematically mistake the absence of a past event for the guarantee of a future one. The turkey fed every morning for a thousand days has no framework for understanding what happens on the thousand and first. Long-term couples navigating HIV risk are not turkeys, but the logical structure of the error is identical.
Viral load complicates this further in ways that do not conform to any intuitive model of accumulated protection. A partner who has been undetectable for six years is not someone whose transmissibility has been decreasing incrementally over those six years in a way that eventually reaches zero. Antiretroviral therapy suppresses the virus to levels below detection thresholds, but suppression is contingent on consistent adherence, on the absence of drug resistance, on the absence of other infections that can cause transient viral blips. The timeline of treatment is not a countdown toward permanent safety. It is a daily maintenance of a condition that must be actively sustained to remain stable.
The emotional weight of shared years does something else too, something less often named. It makes renegotiation feel like accusation. When a couple has operated under an unspoken agreement for years, raising the question of testing, or of viral load confirmation, or of changed sexual behavior, carries the implicit suggestion that the years themselves were built on something suspect. This is why the silence tends to compound rather than resolve. Each year that passes without conversation makes the conversation feel less possible, because initiating it now means accounting for every year it was not initiated before.
The sociologist Anthony Giddens wrote in 1992 about what he called the pure relationship, a modern intimate bond held together not by external obligation but by the continuous emotional satisfaction it provides to both parties. One structural consequence of this model is that anything perceived as threatening the emotional quality of the relationship becomes something both parties have incentive to suppress. Health conversations that introduce uncertainty threaten the felt security of the bond, and so they are deferred, and the deferral itself becomes part of the emotional texture of the relationship, invisible and load-bearing.
What years of shared life actually accumulate is not biological protection but something more like narrative mass, the weight of a shared story that becomes increasingly difficult to revise. The body remains indifferent to that story. Cells do not read the chapters that came before. Every moment of exposure is, from a virological standpoint, a first encounter with the same unchanged question, and the years that felt like answers were only ever the silence before it was asked again.
💉 Love, Risk, and Hidden Truths in Long-Term Bonds
HIV transmission within long-term relationships raises profound questions about trust, communication, and the secret lives partners lead. The intimacy of a committed bond can paradoxically become a space of vulnerability and concealment. These articles explore the psychological and relational landscapes where silence, loyalty, and risk intertwine.
The betrayal and couple secrets
The betrayal within a couple is rarely a single dramatic act but rather a slow erosion of honesty that reshapes the entire emotional architecture of the relationship. Secrets, once embedded in the fabric of a partnership, alter the way intimacy is experienced and shared. Understanding how concealment operates between partners is essential to grasping why health-related truths, including HIV status, so often remain unspoken.
GO TO THE SELECTION: The betrayal and couple secrets
Feeling lonely in a relationship and the loneliness of couples
Feeling lonely while still being in a relationship is one of the most psychologically complex forms of isolation a person can endure. When partners stop truly communicating, invisible walls grow around each individual, creating emotional distance that physical proximity cannot bridge. This relational loneliness is precisely the kind of environment in which critical conversations about sexual health and risk are never had.
GO TO THE SELECTION: Feeling lonely in a relationship and the loneliness of couples
The Conjugal Deception: Where Love Ends and the Performance Begins
The conjugal performance, that daily theater of normalcy and affection maintained for the outside world, often masks profound dysfunctions within the couple’s private reality. When love has quietly dissolved into habit and obligation, partners may continue enacting roles while avoiding any honest confrontation with shared risks. This gap between appearance and truth is a fertile ground for the silence that enables HIV transmission to go unaddressed.
GO TO THE SELECTION: The Conjugal Deception: Where Love Ends and the Performance Begins
Gaslighting: Psychology and Culture
Gaslighting within an intimate relationship creates a pervasive distortion of reality that can leave one partner unable to trust their own perceptions of risk and danger. When one person systematically undermines the other’s concerns, conversations about sexual health or infidelity become almost impossible to initiate or sustain. Recognizing psychological manipulation is therefore a crucial step in understanding how health vulnerability is created and maintained within long-term partnerships.
GO TO THE SELECTION: Gaslighting: Psychology and Culture
Discover Stories That Dare to Tell the Truth
Independent cinema has always been the space where the uncomfortable truths of intimate life are told with honesty and courage. On Indiecinema you will find films that explore love, risk, silence, and the hidden lives we lead beside the people we call our own. Join us and let the stories that matter find you.
👉 EXPLORE THE CATALOG: Watch Indie Films in Streaming
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision

