The Morning You Stopped Looking
You do it every morning without noticing. You lean toward the mirror, toothbrush already working, eyes scanning the surface of your face with the practiced efficiency of someone checking a car for dents before returning it to the rental lot. And then, for just a fraction of a second, you see it — the tongue, pushed forward by reflex or accident, pale or coated or cracked or trembling slightly at the edges — and you look away. Not with disgust, not with fear exactly. With something more familiar than either of those: the specific blankness of a person who has learned, very thoroughly, not to ask certain questions.

That looking away is not accidental. It has been cultivated.
There is a man who spends three years unable to sleep more than four hours a night. His body has been sending signals with the insistence of a neighbor banging on the wall — a tongue so swollen it bears the pressed imprints of his teeth along both sides, a thin white film that never quite disappears no matter how many times he brushes, a center line running down the middle like a dry riverbed. He shows it to his doctor once. The doctor looks briefly, says nothing is wrong, and moves on to the blood pressure cuff. The man goes home and does not look again for years. Not because he is incurious. Because he has been taught that what he sees with his own eyes, in his own mouth, in his own mirror, does not constitute knowledge.
This is the epistemological wound at the center of modern health culture: the systematic devaluation of the body’s own testimony.
Michel Foucault, in The Birth of the Clinic published in 1963, traced with surgical precision the moment when Western medicine reorganized itself around the clinical gaze — the physician’s eye, the physician’s ear, the physician’s interpretation replacing the patient’s experience as the primary source of medical truth. Before the late eighteenth century, Foucault argues, disease was understood through the patient’s narration of their own suffering. After the reorganization of hospital medicine in post-Revolutionary France, the body became an object to be read by an expert, and the person inhabiting it became, in a meaningful sense, a bystander to their own condition. Two hundred and sixty years of institutional reinforcement later, we have internalized this so completely that looking at our own tongue in the mirror and finding it meaningful feels almost presumptuous. Almost like trespassing.
And yet the tongue has been considered a diagnostic landscape for over two thousand years across cultures that had no contact with each other. The classical Chinese medical texts, the Huangdi Neijing compiled across centuries before the common era, describe tongue observation as a primary diagnostic method with a specificity that took Western medicine until the late twentieth century to even begin acknowledging. Ayurvedic practitioners in India were reading tongue color, texture, and coating as indices of digestive and systemic health before the Roman Empire existed. These were not superstitions. They were careful, cumulative, empirically refined observations made by people who had nothing to gain from inventing correlations that did not exist.
What we have lost is not the information. The tongue has not stopped speaking. It is producing the same signals it always produced, the same geographic variations, the same subtle colors, the same textures that map, with more fidelity than most people are comfortable accepting, onto what is happening several layers beneath the skin. What we have lost is the habit of looking. And more precisely, the conviction that looking is allowed — that the body’s surface is a legitimate text, that you are entitled to read it, that you do not need a credential to notice that something in your own interior has changed.
Every morning, the mirror waits. And every morning, most of us look at our eyes, our skin, our hair — the social surfaces, the ones that face outward — and let the tongue retreat back behind the teeth, unread.
The Map That Predates the Doctor
There is a moment, familiar to almost anyone who has sat in a doctor’s waiting room, when you realize that the person across from you — clipboard in hand, eyes moving between screen and stethoscope — is reading you through instruments that stand between them and your body like a kind of translation device. The body becomes data. The data becomes diagnosis. Somewhere in that translation, something that was yours gets handed over to a language you do not speak.
This is not a modern problem. It is, in fact, the problem that certain medical traditions spent thousands of years trying to solve from the opposite direction — by reading the body’s interior through its surfaces, by treating the visible as a direct messenger from the invisible, by refusing to separate the territory from the map.
The Huangdi Neijing, the foundational classical Chinese medical text compiled approximately around 200 BCE and attributed in legendary terms to the Yellow Emperor himself, contains among its vast architecture of systematic observation one of the earliest documented frameworks for tongue diagnosis. What is described there is not a metaphor and not a mystical inference. It is a clinical methodology: specific regions of the tongue’s surface correspond to specific organ systems — the tip to the heart and lungs, the middle body to the spleen and stomach, the root to the kidneys, the lateral edges to the liver and gallbladder. Coating color, moisture, the presence or absence of cracks, the vitality of what Chinese medicine calls the shen visible in the tongue’s overall appearance — all of it readable, all of it meaningful, all of it part of a coherent epistemology that had been refined across centuries of recorded observation before European medicine had begun to systematize anything resembling it.
Ayurvedic practitioners working within the framework that crystallized in texts like the Charaka Samhita, composed somewhere between the first and second centuries CE, approached the tongue from a structurally similar but philosophically distinct position. The tongue was read as terrain — a landscape shaped by the relative dominance of vata, pitta, and kapha, the three doshas that in Ayurvedic theory govern all physiological and psychological function. A dry, rough tongue with cracks suggested vata excess; a red or inflamed tongue with yellowish coating pointed toward pitta imbalance; a pale, swollen tongue coated in white pointed to kapha predominance. The physician did not require a laboratory. The physician required attention — a trained, sustained, intimate attention to what the body was already showing.
What Foucault identified in The Birth of the Clinic, published in 1963, was the precise historical moment when this kind of attention began to be replaced by something else. He traced how the gaze of Western medicine shifted, particularly through the late eighteenth and early nineteenth centuries, from the patient’s experience of illness to the physician’s interpretation of lesions, tissues, measurable deviations from statistical norms. The body became an object to be decoded from outside rather than a living interior to be listened to from within. This was not simply a scientific advancement. It was a reorganization of power — a decision, encoded in institutional structures, about whose knowledge counts and whose does not.
The largely forgotten humoral physicians of seventeenth-century Europe were still operating within a tradition that included tongue observation as meaningful diagnostic practice. Practitioners working in the lineage of Galenic medicine read the tongue’s color and moisture as indicators of the body’s dominant humor, its thermal state, its fundamental constitution. That tradition was not superseded because it was proven useless. It was erased because the new clinical model required a cleaner epistemological field — and erasure is always easier when the knowledge being erased belongs to systems that have already been marked, for other reasons, as peripheral, foreign, or pre-scientific.
The question of who benefits from that erasure is not rhetorical.
What the Tongue Actually Carries
There is a man who has been waking at three in the morning for six months. Not from noise, not from worry he can name. Something pulls him upward from sleep, and he lies in the dark with a dull ache behind his right rib, a taste in his mouth like copper and old wood. He does not go to a doctor. He assumes it is stress, bad wine, the particular exhaustion of middle age. His tongue, if he had thought to look at it, would have told him something urgent: a thick yellow coating concentrated along the right lateral edge, the flesh beneath it faintly purple in the morning light, the tip cracked and dry as paper in August. He was not reading it. He did not know it was speaking.
The coating that forms on the tongue’s surface is not simply accumulated bacteria or poor oral hygiene, though it involves both. It is a metabolic signature. In healthy digestive function, a thin white coating — nearly transparent, evenly distributed — reflects a balanced microbial environment and adequate enzymatic activity along the gastrointestinal tract. When that coating thickens, yellows, or develops texture resembling curd or paste, it maps onto a disruption in the digestive process: bacterial overgrowth, sluggish bile production, or intestinal inflammation. Research published in the Journal of Clinical Gastroenterology has shown measurable correlations between tongue coating composition and the microbial diversity of the gut, confirming what observational medicine had noticed for centuries. A white coating that is thick and wet suggests dampness and impaired fluid metabolism. A yellow coating, particularly when concentrated and sticky, points toward heat accumulation and biliary stress. A coating that is absent entirely — a tongue stripped bare and raw-looking — signals something different and often more alarming: depletion, a body that has exhausted its capacity to generate even the surface layer of normal metabolic activity.
Beneath the coating lies what diagnosticians call the body of the tongue, the living flesh itself, and its color carries a different register of information. The normal color is described as a particular shade: pale red or fresh pink, neither too deep nor too washed out. Redness that deepens toward crimson, especially when it concentrates at the tip, tends to indicate chronic inflammatory states or cardiovascular stress, the circulatory system under pressure it cannot adequately resolve. A purplish or bluish tinge across the body of the tongue, or visible purple veins on the underside when the tongue is lifted, reflects circulatory stagnation — blood moving sluggishly, oxygen delivery compromised, a pattern that appears in chronic pain conditions, in people with long-standing depression, in those whose hands and feet are always cold regardless of the season. Pallor in the tongue’s body, a washed-out pinkish white, tends to accompany anemia, low thyroid function, or adrenal insufficiency — conditions where the body is conserving rather than generating, where energy is being rationed at a cellular level.
Maurice Merleau-Ponty argued in his Phenomenology of Perception, published in 1945, that the body is not an instrument we operate from the outside, not an object we happen to inhabit, but the very medium through which we exist and encounter the world at all. To observe one’s own body carefully, then, is not vanity and not hypochondria. It is a form of knowing that is prior to and more immediate than any abstract reasoning. When you look at your tongue each morning, you are not performing a medical examination in the clinical sense. You are engaging in something phenomenological — meeting the body on its own terms, in its own language, before translation into symptoms and diagnoses strips away the specificity of what it is actually saying.
The geographic mapping of organ systems onto the tongue’s surface extends this logic into something almost architectural.
The Cultural Silencing of Interior Knowledge
She had been watching her tongue for three weeks. Every morning, the same ritual: lean toward the mirror, extend the tongue, note the color, the coating, the way the edges had begun to corrugate slightly on the left side. She had filled half a notebook with careful observations, cross-referencing them with fatigue patterns, digestive episodes, the strange heaviness behind her right eye that came and went without explanation. She brought all of this to her physician, the notebook included. He glanced at the tongue briefly, the way you glance at a clock you have no intention of reading, and said the words that functioned less as a medical assessment than as a boundary enforcement: “That’s not really how we diagnose things.”
What he meant, though he would never have put it this way, was that her knowledge did not count as knowledge. Not because it was inaccurate. Not because the observations were flawed. But because they had been generated outside the institutional apparatus that decides what evidence is allowed to be called evidence.
Ivan Illich understood this mechanism with almost brutal clarity. In 1974, when Medical Nemesis arrived as something between a sociological study and an act of intellectual aggression, Illich named what he called iatrogenesis — not merely the harm caused by medical error, but the deeper, structural harm caused by medicine’s colonization of the individual’s capacity to understand and interpret their own body. The medicalization of health, he argued, does not simply treat illness. It systematically dismantles the person’s ability to perceive, interpret, and respond to their own interior signals. It creates dependency not as a side effect but as an architecture. The patient is trained, across decades of institutional encounter, to distrust exactly the kind of careful, embodied, longitudinal self-observation that the woman with the notebook had been practicing.
Pierre Bourdieu would have recognized the scene immediately. His concept of symbolic capital — elaborated across works like Distinction and The Logic of Practice — explains that bodies of knowledge are not legitimized according to their truth value but according to their proximity to institutional power. Traditional Chinese medicine carries millennia of systematic clinical refinement, cross-cultural replication, and empirical observation. Ayurvedic tongue diagnosis predates the stethoscope by roughly three thousand years. And yet both exist in the Western medical imagination as folklore, as cultural curiosity, as the kind of thing that gets a polite nod before the real consultation begins. The dismissal is not scientific. It is sociological. It is the performance of epistemic authority, which is always also the performance of who belongs and who does not.
What makes this particularly strange, when you sit with it long enough, is that tongue observation is not mystical. It is material. It is the reading of a visible, accessible, perpetually renewing surface of tissue that responds in documented, reproducible ways to internal physiological states. The coating changes with gut flora disruption. The color shifts with circulatory and oxygenation patterns. The surface texture responds to inflammatory states. These are not metaphors. They are mechanisms. The ancient practitioners who developed these diagnostic frameworks were not operating on faith. They were operating on something closer to what we now call longitudinal clinical observation — the slow accumulation of pattern recognition across thousands of cases, refined across generations.
But pattern recognition developed outside a laboratory, documented in languages other than the language of randomized controlled trials, transmitted through lineages rather than journals, does not qualify for entry. The gate is not about truth. The gate is about the form in which truth arrives, and who trained the gatekeeper.
She closed her notebook. She thanked him. She walked out into a world that had been teaching her, her entire life, to stop trusting what she could see with her own eyes.
Learning to Read the Face of the Interior
There is a particular quality of light that works best for this — morning light, before coffee, before the first word spoken aloud to anyone. You stand at the bathroom mirror, open your mouth, and look. Not scan, not glance, not confirm what you already expect to see. Look, in the way that Simone Weil meant when she wrote that attention is the rarest and purest form of generosity, a complete suspension of the self so that reality can enter. Weil was speaking of prayer and of learning, but the structure she described applies with uncomfortable precision to this small daily act: to truly attend to something is to allow it to inform you rather than confirm you.
Most people who try this for the first time see very little. A pink surface, perhaps some texture, the vague geography of a body part they have never considered an organ of communication. But the tongue does not reveal itself in a single sitting. It asks for return, for the accumulation of mornings, for the patience that belongs to a different relationship with time than the one modern life has trained into most bodies. After two weeks, something shifts. A coating that seemed uniform begins to show its borders. A region on the left side appears consistently drier, thicker, less vital than the rest. The color at the root is not the same as the color at the tip. None of this felt true on the first day. It becomes true only through repetition, through the slow construction of a baseline against which deviation becomes visible.
This is where the experience turns strange, and for some people, briefly unsettling. Because the patterns that emerge are not new. The fatigue that pools in a particular quadrant of the tongue on Monday mornings — you have felt that fatigue for years. The pale, swollen edges that appear in November and disappear in April — the winters have always been harder, in ways you could never quite name to a doctor in a seven-minute appointment. The body, it becomes clear, has not been withholding information. It has been transmitting continuously, in a language that required only a different quality of looking to become legible.
Paul Ricoeur wrote in Oneself as Another that the self is not a given but a task — something arrived at through interpretation, through the sustained effort of reading the signs that experience leaves in the body and in memory. What daily tongue observation offers, at its most serious, is a practice of exactly this kind: a hermeneutics of the interior, a discipline of interpretation that is also, slowly, a discipline of self-recognition. The tongue does not tell you who you are in any final sense. It tells you where you are, metabolically, emotionally, seasonally, and it does so without flattery or concealment.
There is something almost ethically disorienting in this realization, once it arrives. To understand that the body has been consistent in its signals across years or even decades — that the patterns were always present, always coherent, always pointing — is to confront the question of what it has meant to not look. Not from negligence exactly, and not from ignorance, but from a kind of trained inattention, a cultural arrangement in which the body speaks and the person it inhabits learns, very early and very thoroughly, to wait for an external authority to do the listening. The tongue has been a text all along, patient and undemanding, requiring nothing more than the willingness to stand still for a moment and receive what it has never, not once, stopped saying.
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision
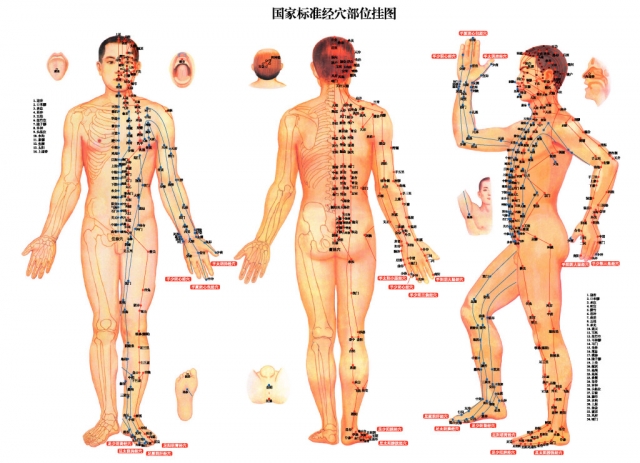
🌿 Ancient Maps of the Body’s Inner Wisdom
The tongue is not merely a muscle — in traditional medicine, it is a living map of the body’s deepest energies, organs, and imbalances. To understand what the tongue reveals, one must first grasp the intricate systems that govern life force, energetic channels, and the rhythms of the organs themselves. These articles deepen the journey inward.
The Organ Clock: Why Every Organ Has Its Time of Peak and Low Energy
Just as the tongue reflects the state of each organ at any given moment, the Organ Clock teaches us that every organ pulses with its own rhythm of peak vitality and depletion throughout the day. Understanding these energetic tides allows us to read the body’s signals — including those written on the tongue — with far greater precision. Time, in traditional medicine, is not abstract but deeply biological and energetic.
GO TO THE SELECTION: The Organ Clock: Why Every Organ Has Its Time of Peak and Low Energy
The 12 Energetic Channels: The Secret Map of Meridians in Body
The meridian system forms the invisible infrastructure through which organ health is communicated to the surface of the body, including the tongue. Each zone of the tongue corresponds to a specific meridian pathway, making the map of channels essential knowledge for any serious student of tongue diagnosis. This article traces that secret cartography with clarity and depth.
GO TO THE SELECTION: The 12 Energetic Channels: The Secret Map of Meridians in Body
Vital Breath: if Your Qi is Blocked, Weak, or Scattered
A tongue that appears pale, trembling, or lacking vitality often signals that Qi itself is compromised — blocked in its flow, insufficient in its quantity, or scattered across the body without direction. Understanding the nature of Qi and its various dysfunctions is foundational to interpreting what the tongue’s color, moisture, and coating are actually communicating. This article offers a precise and illuminating guide to the breath that animates all living systems.
GO TO THE SELECTION: Vital Breath: if Your Qi is Blocked, Weak, or Scattered
The Dance of Yin and Yang: Harmony Between Opposing Forces
The tongue’s two hemispheres, its color gradients, and the balance between moisture and dryness all speak the ancient language of Yin and Yang in constant negotiation within the body. When these opposing forces fall out of harmony, the tongue becomes one of the first mirrors to reflect that inner discord. This article explores the philosophical and practical dimensions of that eternal dance between shadow and light.
GO TO THE SELECTION: The Dance of Yin and Yang: Harmony Between Opposing Forces
🎬 Explore the Inner Worlds of Independent Cinema
If these hidden maps of the body and spirit have stirred something in you, Indiecinema streaming invites you to continue the journey through the language of film. Discover independent and arthouse cinema that dares to explore consciousness, healing, and the mysteries of human existence — stories that conventional screens rarely tell. Join Indiecinema and let the screen become your next portal inward.
👉 EXPLORE THE CATALOG: Watch Indie Films in Streaming
A vision curated by a filmmaker, not an algorithm
In this video I explain our vision

